School of Population Health and Environmental Sciences, Guy's Campus, King's College London, London, United Kingdom.
National Institute for Health Research Biomedical Research Centre at Guy's and St Thomas' Hospitals London, Great Maze Pond, London, United Kingdom.
PLoS One. 2020 Dec 31;15(12):e0244764. doi: 10.1371/journal.pone.0244764. eCollection 2020.
Sepsis is a growing concern for health systems, but the epidemiology of sepsis is poorly characterised. We evaluated sepsis recording across primary care electronic records, hospital episodes and mortality registrations.
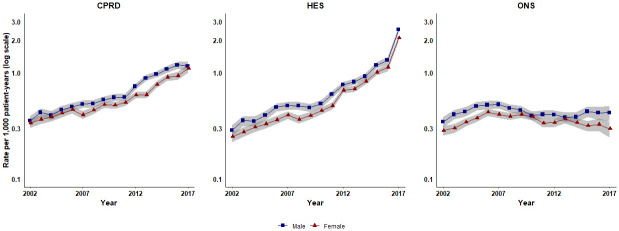
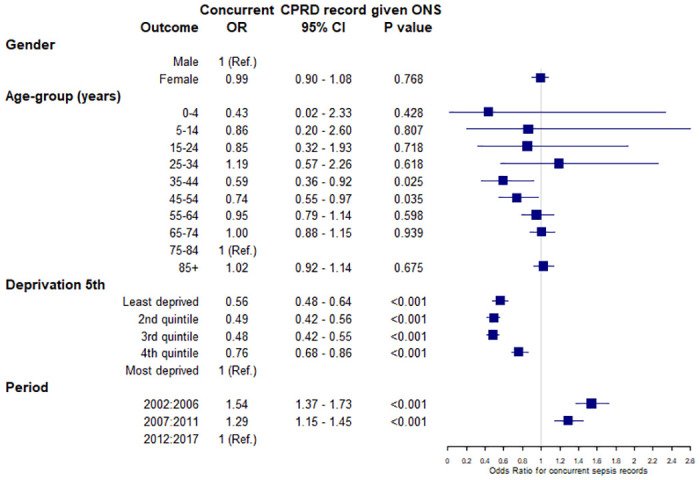
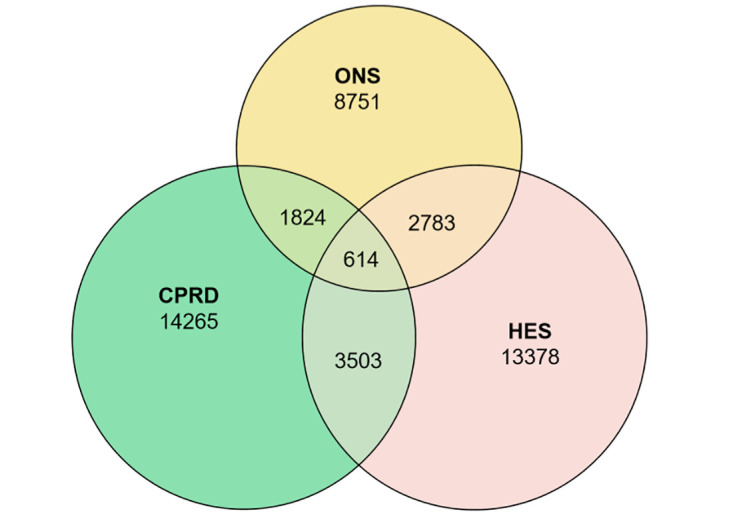
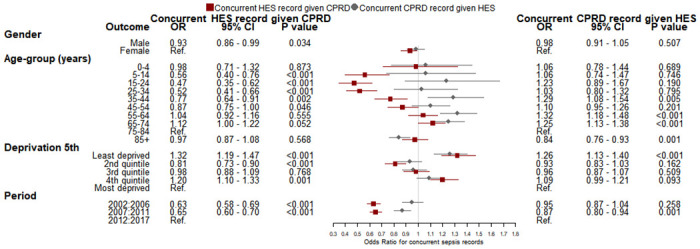
Cohort study including 378 general practices in England from Clinical Practice Research Datalink (CPRD) GOLD database from 2002-2017 with 36,209,676 patient-years of follow-up with linked Hospital Episode Statistics (HES) and Office for National Statistics (ONS) mortality registrations. Incident sepsis episodes were identified for each source. Concurrent records from different sources were identified and age-standardised and age-specific incidence rates compared. Logistic regression analysis evaluated associations of gender, age-group, fifth of deprivation and period of diagnosis with concurrent sepsis recording. There were 20,206 first episodes of sepsis from primary care, 20,278 from HES and 13,972 from ONS. There were 4,117 (20%) first HES sepsis events and 2,438 (17%) mortality records concurrent with incident primary care sepsis records within 30 days. Concurrent HES and primary care records of sepsis within 30 days before or after first diagnosis were higher at younger or older ages and for patients with the most recent period of diagnosis. Those diagnosed during 2007:2011 were less likely to have a concurrent HES record given CPRD compared to those diagnosed during 2012-2017 (odd ratio 0.65, 95% confidence interval 0.60-0.70). At age 85 and older, primary care incidence was 5.22 per 1,000 patient years (95% CI 1.75-11.97) in men and 3.55 (0.87-9.58) in women which increased to 10.09 (4.86-18.51) for men and 7.22 (2.96-14.72) for women after inclusion of all three sources.
Explicit recording of 'sepsis' is inconsistent across healthcare sectors with a high proportion of non-concurrent records. Incidence estimates are higher when linked data are analysed.
败血症是卫生系统日益关注的问题,但败血症的流行病学特征描述不佳。我们评估了初级保健电子记录、医院发病和死亡率登记处中败血症的记录情况。
这项包括英格兰 378 个普通实践的队列研究,数据来源于 2002 年至 2017 年的临床实践研究数据链接(CPRD)GOLD 数据库,共 36209676 患者年的随访记录,这些记录与医院发病统计(HES)和国家统计局(ONS)死亡率登记处相关联。从每个来源确定了败血症的发病情况。确定了不同来源的同时记录,并对其进行了年龄标准化和年龄特异性发病率比较。逻辑回归分析评估了性别、年龄组、贫困程度的五分之一和诊断时期与同时记录败血症之间的关联。从初级保健中发现了 20206 例首次败血症发作,从 HES 中发现了 20278 例,从 ONS 中发现了 13972 例。在 30 天内,有 4117 例(20%)首次 HES 败血症事件和 2438 例(17%)死亡记录与首次初级保健败血症记录同时发生。在年龄较小或较大时,以及在最近诊断时期的患者中,30 天内之前或之后首次诊断的 HES 和初级保健败血症记录的同时发生频率更高。与 2012 年至 2017 年相比,2007 年至 2011 年期间诊断的患者发生 HES 记录的可能性更低(比值比 0.65,95%置信区间 0.60-0.70)。在 85 岁及以上的男性中,每 1000 名患者年的初级保健发病率为 5.22(95%CI 1.75-11.97),女性为 3.55(0.87-9.58),而当包括所有三个来源时,男性发病率为 10.09(4.86-18.51),女性发病率为 7.22(2.96-14.72)。
在医疗保健领域中,“败血症”的明确记录并不一致,有很大比例的非同时记录。当分析链接数据时,发病率估计值更高。