London School of Hygiene and Tropical Medicine, London WC1E 7HT, UK.
BMJ. 2013 May 20;346:f2350. doi: 10.1136/bmj.f2350.
To determine the completeness and diagnostic validity of myocardial infarction recording across four national health record sources in primary care, hospital care, a disease registry, and mortality register.
Cohort study.
21 482 patients with acute myocardial infarction in England between January 2003 and March 2009, identified in four prospectively collected, linked electronic health record sources: Clinical Practice Research Datalink (primary care data), Hospital Episode Statistics (hospital admissions), the disease registry MINAP (Myocardial Ischaemia National Audit Project), and the Office for National Statistics mortality register (cause specific mortality data).
One country (England) with one health system (the National Health Service).
Recording of acute myocardial infarction, incidence, all cause mortality within one year of acute myocardial infarction, and diagnostic validity of acute myocardial infarction compared with electrocardiographic and troponin findings in the disease registry (gold standard).
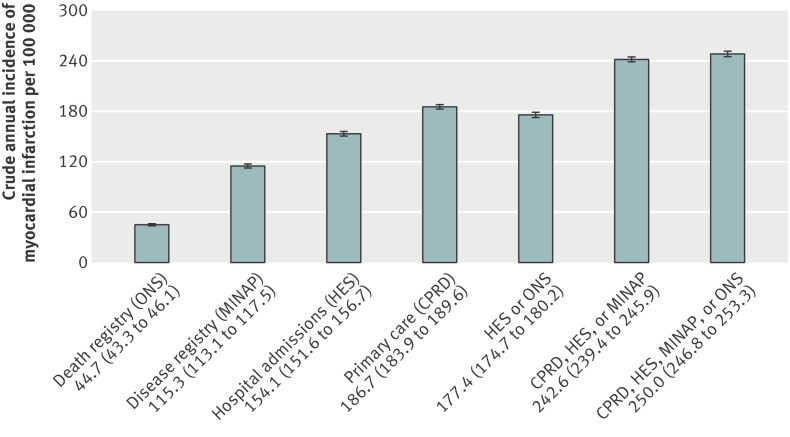
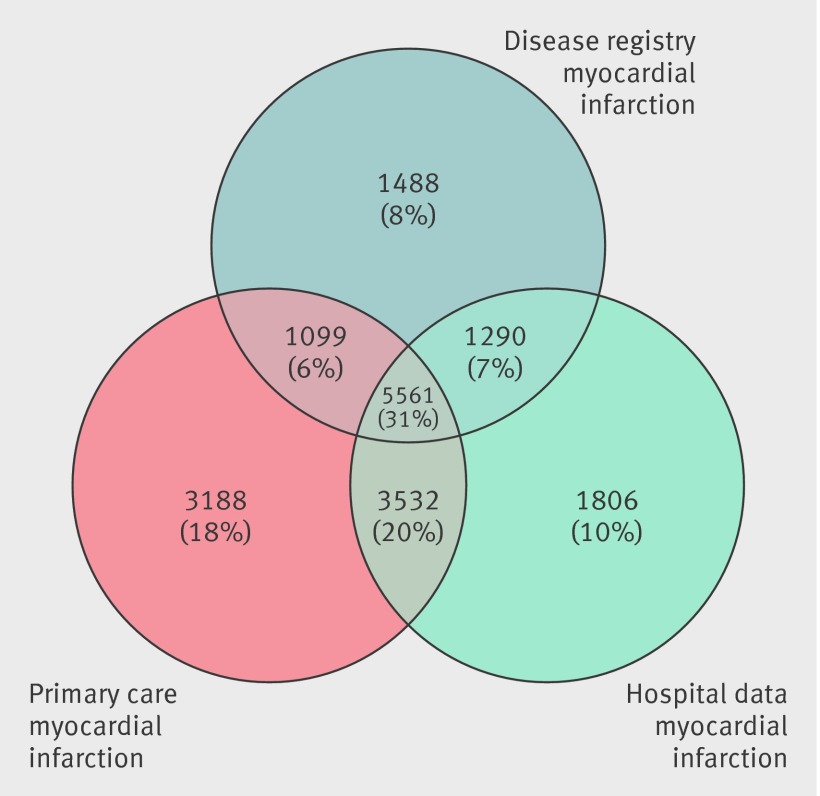
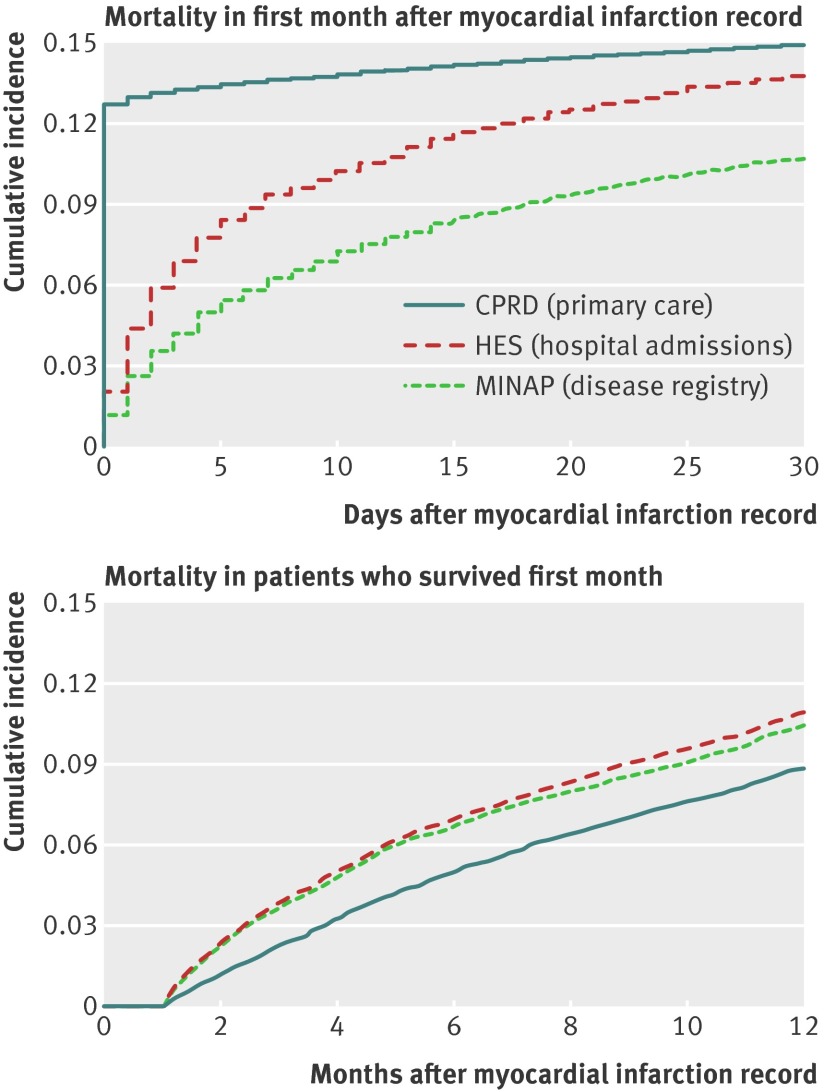
Risk factors and non-cardiovascular coexisting conditions were similar across patients identified in primary care, hospital admission, and registry sources. Immediate all cause mortality was highest among patients with acute myocardial infarction recorded in primary care, which (unlike hospital admission and disease registry sources) included patients who did not reach hospital, but at one year mortality rates in cohorts from each source were similar. 5561 (31.0%) patients with non-fatal acute myocardial infarction were recorded in all three sources and 11 482 (63.9%) in at least two sources. The crude incidence of acute myocardial infarction was underestimated by 25-50% using one source compared with using all three sources. Compared with acute myocardial infarction defined in the disease registry, the positive predictive value of acute myocardial infarction recorded in primary care was 92.2% (95% confidence interval 91.6% to 92.8%) and in hospital admissions was 91.5% (90.8% to 92.1%).
Each data source missed a substantial proportion (25-50%) of myocardial infarction events. Failure to use linked electronic health records from primary care, hospital care, disease registry, and death certificates may lead to biased estimates of the incidence and outcome of myocardial infarction.
NCT01569139 clinicaltrials.gov.
确定在初级保健、医院护理、疾病登记处和死亡登记处的四个国家健康记录来源中,心肌梗死记录的完整性和诊断有效性。
队列研究。
2003 年 1 月至 2009 年 3 月期间,英格兰有 21482 名急性心肌梗死患者,从四个前瞻性收集的、链接的电子健康记录来源中确定:临床实践研究数据链接(初级保健数据)、医院事件统计(医院入院)、疾病登记处 MINAP(心肌缺血国家审计项目)和国家统计局死亡登记处(特定原因死亡率数据)。
一个国家(英国),一个卫生系统(国民保健服务)。
急性心肌梗死的记录、发生率、急性心肌梗死后一年内的全因死亡率,以及与疾病登记处的心电图和肌钙蛋白发现相比的急性心肌梗死的诊断有效性(金标准)。
在初级保健、医院入院和登记处来源中确定的患者中,危险因素和非心血管并存疾病相似。在初级保健中记录的急性心肌梗死患者的即时全因死亡率最高,(与医院入院和登记处来源不同)包括未到达医院的患者,但在一年时,每个来源的队列的死亡率相似。5561(31.0%)例非致命性急性心肌梗死患者在所有三个来源中记录,11482(63.9%)例至少在两个来源中记录。与使用所有三个来源相比,使用一个来源会低估急性心肌梗死的发病率 25-50%。与疾病登记处定义的急性心肌梗死相比,初级保健中记录的急性心肌梗死的阳性预测值为 92.2%(95%置信区间 91.6%至 92.8%),在医院入院中的为 91.5%(90.8%至 92.1%)。
每个数据源都遗漏了相当一部分(25-50%)的心肌梗死事件。未能使用初级保健、医院护理、疾病登记处和死亡证明的链接电子健康记录可能导致对心肌梗死的发病率和结果产生偏差估计。
NCT01569139 clinicaltrials.gov。