Department of Pediatric Hematology, Oncology and Stem Cell Transplantation, University Hospital of Regensburg, Franz-Josef-Strauss Allee 11, 93053, Regensburg, Germany.
Int J Med Sci. 2021 Jan 1;18(1):137-149. doi: 10.7150/ijms.48393. eCollection 2021.
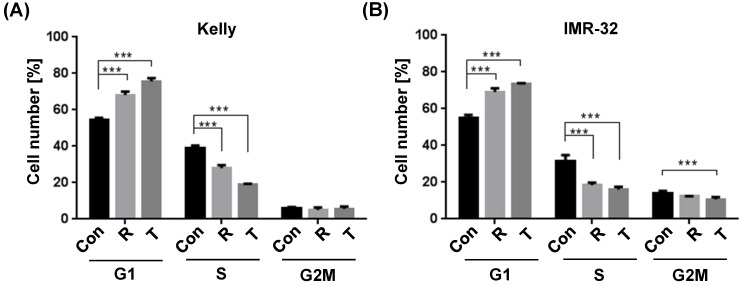
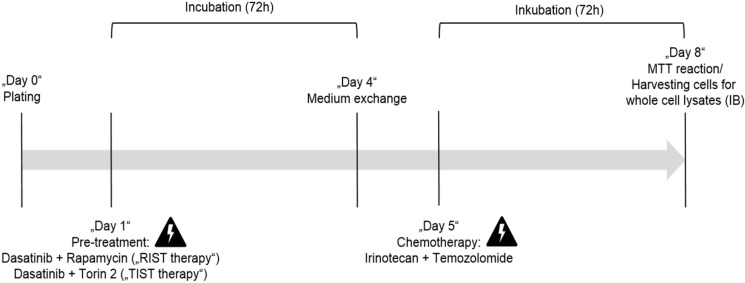
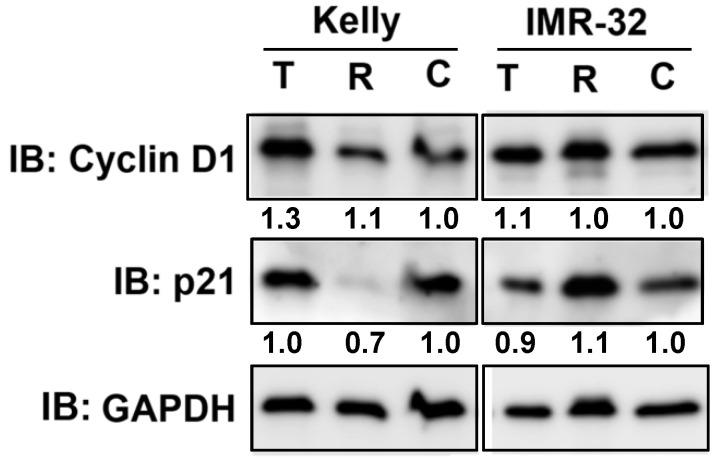
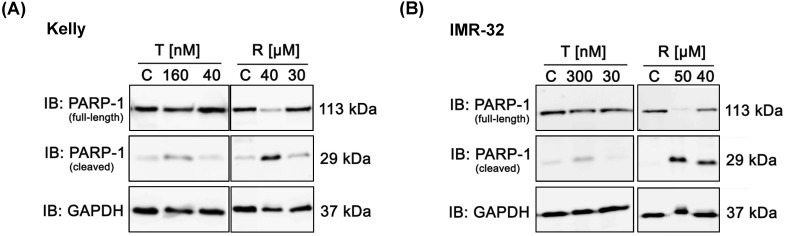
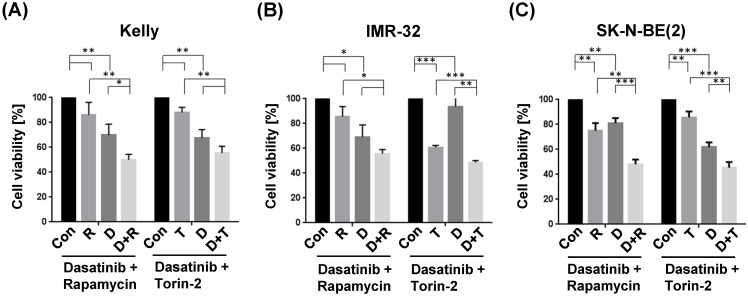
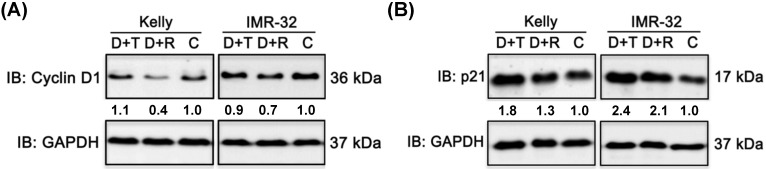
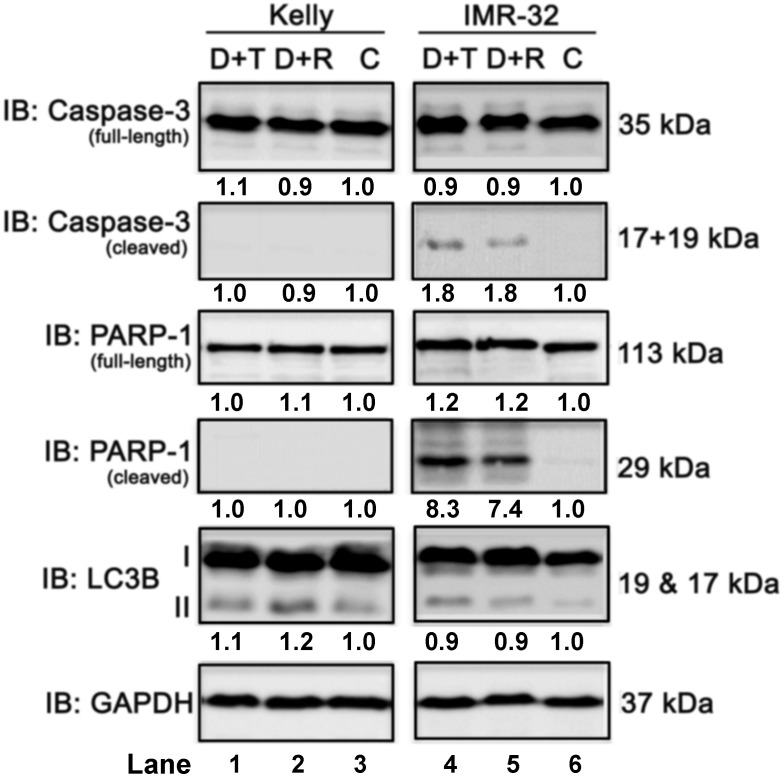
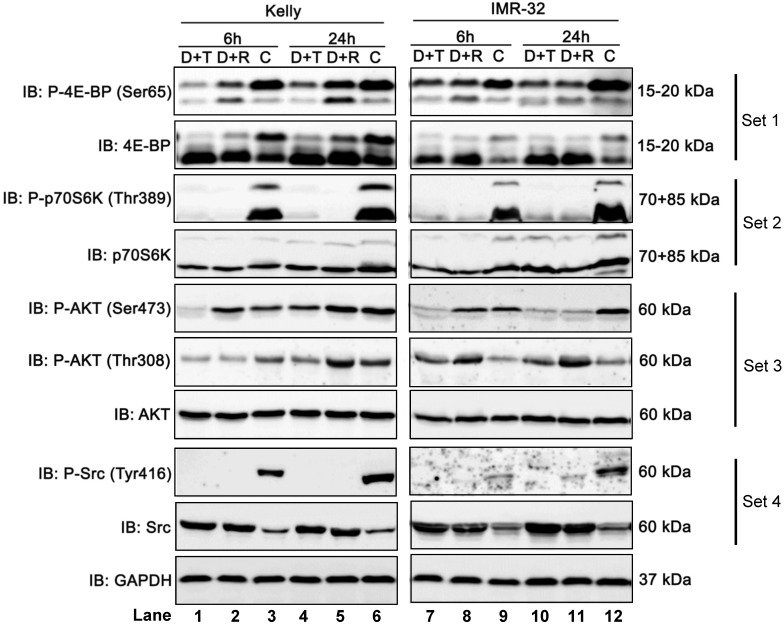
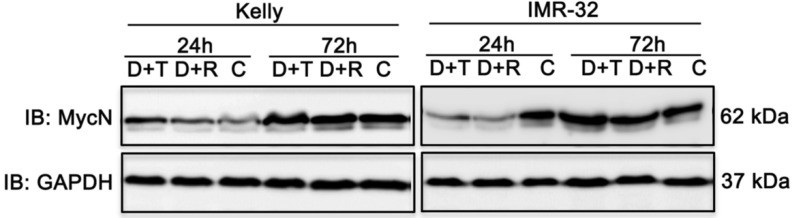
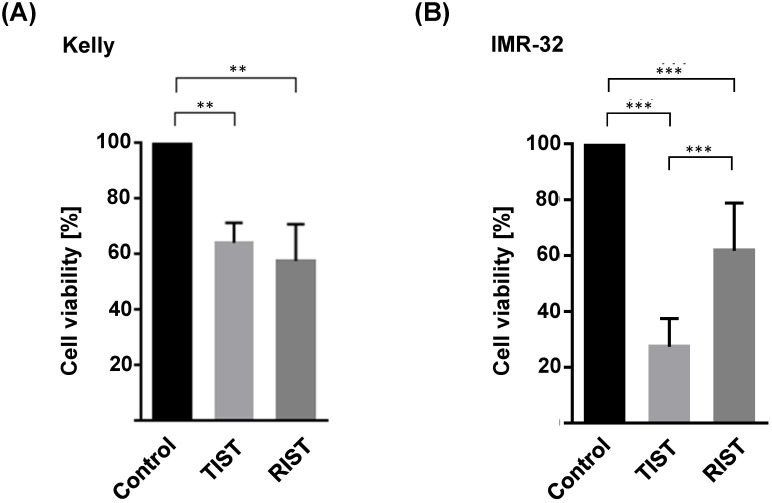
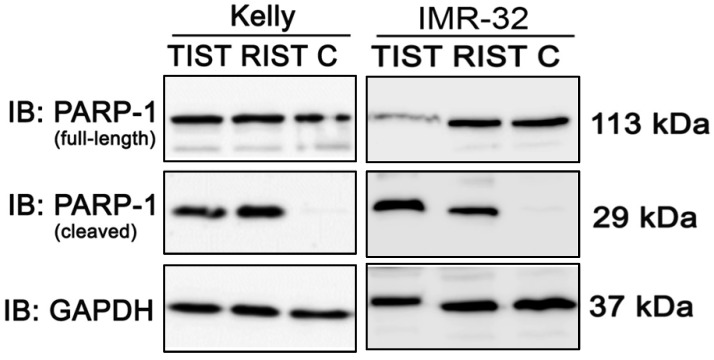
The prognosis for patients with relapsed or refractory high-risk neuroblastoma remains dismal and novel therapeutic options are urgently needed. The RIST treatment protocol has a multimodal metronomic therapy design combining molecular-targeted drugs (Rapamycin and Dasatinib) with chemotherapy backbone (Irinotecan and Temozolomide), which is currently verified in a phase II clinical trial (NCT01467986). With the availability of novel and more potent ATP competitive mTOR inhibitors, we expect to improve the RIST combination therapy. By comparing the IC values of Torin-1, Torin-2, AZD3147 and PP242 we established that only Torin-2 inhibited cell viability of all three MycN-amplified neuroblastoma cell lines tested at nanomolar concentration. Single treatment of both mTOR inhibitors induced a significant G cell cycle arrest and combination treatment with Dasatinib reduced the expression of cell cycle regulator cyclin D1 or increased the expression of cell cycle inhibitor p21. The combinatorial index depicted for both mTOR inhibitors a synergistic effect with Dasatinib. Interestingly, compared to Rapamycin, the combination treatment with Torin-2 resulted in a broader mTOR pathway inhibition as indicated by reduced phosphorylation of AKT (Thr308, Ser473), 4E-BP (Ser65), and S6K (Thr389). Furthermore, substituting Rapamycin in the modified multimodal RIST protocol with Torin-2 reduced cell viability and induced apoptosis despite a significant lower Torin-2 drug concentration applied. The efficacy of nanomolar concentrations may significantly reduce unwanted immunosuppression associated with Rapamycin. However, at this point we cannot rule out that Torin-2 has increased toxicity due to its potency in more complex systems. Nonetheless, our results suggest that including Torin-2 as a substitute for Rapamycin in the RIST protocol may represent a valid option to be evaluated in prospective clinical trials for relapsed or treatment-refractory high-risk neuroblastoma.
对于复发或难治性高危神经母细胞瘤患者,预后仍然不容乐观,急需新的治疗选择。RIST 治疗方案采用多模式节拍式治疗设计,将分子靶向药物(雷帕霉素和达沙替尼)与化疗骨干(伊立替康和替莫唑胺)相结合,目前正在一项 II 期临床试验中进行验证(NCT01467986)。随着新型、更有效的 ATP 竞争性 mTOR 抑制剂的出现,我们期望改善 RIST 联合治疗。通过比较 Torin-1、Torin-2、AZD3147 和 PP242 的 IC 值,我们发现只有 Torin-2 在纳摩尔浓度下抑制了所有三种 MycN 扩增神经母细胞瘤细胞系的细胞活力。两种 mTOR 抑制剂的单独治疗均诱导显著的 G1 细胞周期停滞,与达沙替尼联合治疗降低了细胞周期调节剂 cyclin D1 的表达或增加了细胞周期抑制剂 p21 的表达。两种 mTOR 抑制剂的组合指数均显示与达沙替尼具有协同作用。有趣的是,与雷帕霉素相比,Torin-2 与 Torin-2 的联合治疗导致更广泛的 mTOR 通路抑制,表现为 AKT(Thr308、Ser473)、4E-BP(Ser65)和 S6K(Thr389)的磷酸化减少。此外,尽管应用的 Torin-2 药物浓度显著降低,但在改良的多模式 RIST 方案中用 Torin-2 替代雷帕霉素可降低细胞活力并诱导细胞凋亡。纳摩尔浓度的疗效可能会显著降低与雷帕霉素相关的不必要的免疫抑制作用。然而,目前我们不能排除 Torin-2 由于其在更复杂系统中的效力而增加了毒性。尽管如此,我们的结果表明,在 RIST 方案中用 Torin-2 替代雷帕霉素可能是一种有前途的治疗选择,值得在复发或治疗抵抗性高危神经母细胞瘤的前瞻性临床试验中进行评估。