Department of Hepatobiliary and Pancreatic Surgery, First Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, 310003, China.
Department of Gynecologic Oncology, Women's Hospital, School of Medicine, Zhejiang University, Hangzhou, 310006, China.
BMC Surg. 2021 Jan 4;21(1):4. doi: 10.1186/s12893-020-01019-9.
Mesentericoportal vein (MPV) resection in pancreatic ductal adenocarcinoma (PDAC) surgery has become a common procedure. A few studies had described the use of falciform ligament (FL) for MPV reconstruction and received encouraging preliminary effects.
This study was designed to explore the feasibility and efficacy of this technique compared with others.
Patients who underwent pancreaticoduodenectomy (PD) with MPV resection for PDAC from 2009 to 2018 were enrolled. Medical records were retrospectively reviewed, MPV reconstructions using FL were distinguished and compared with other techniques.
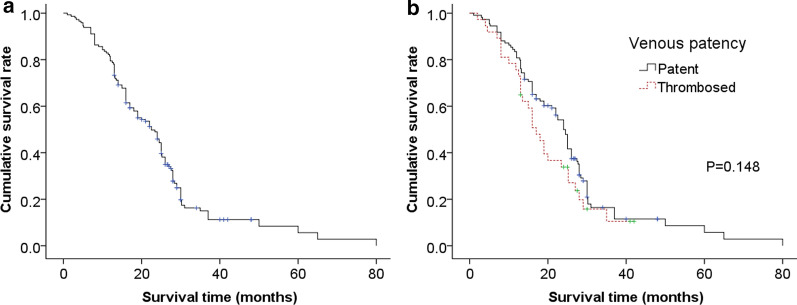
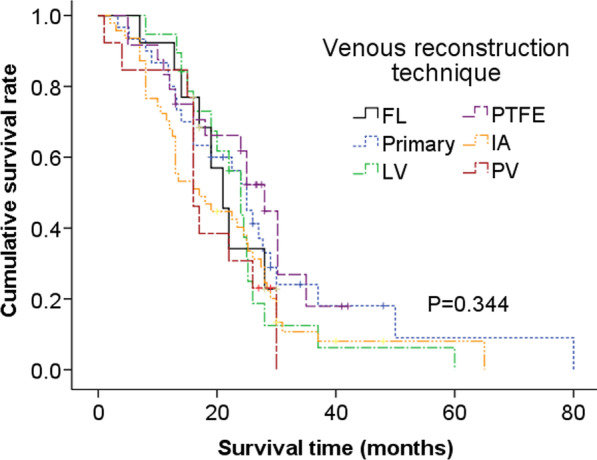
146 patients underwent MPV reconstruction, and 13 received FL venoplasty. Other reconstruction techniques included primary end-to-end anastomosis (primary, n = 30), lateral venorrhaphy (LV, n = 19), polytetrafluoroethylene conduit interposition (PTFE, n = 24), iliac artery (IA) allografts interposition (n = 47), and portal vein (PV) allografts interposition (n = 13). FL group holds the advantages of shortest operation time (p = 0.023), lowest blood loss (p = 0.109), and shortest postoperative hospital stay (p = 0.125). The grouped patency rates of FL, primary, LV, PTFE, IA, and PV were 100%, 90%, 68%, 54%, 68%, and 85% respectively. Comparison displayed that FL had the highest patency rate (p = 0.008) and lowest antiplatelet/anticoagulation proportion (p = 0.000). Complications and long-term survival were similar among different techniques. The median survival time of patent group (24.0 months, 95% CI: 22.0-26.0) was much longer than that of the thrombosed (17.0 months, 95% CI: 13.7-20.3), though without significant difference (P = 0.148).
PD with MPV resection and reconstruction by FL is safe, feasible, and efficacious, it might provide a potential benefit for patients.
肠系膜门静脉(MPV)切除术在胰腺导管腺癌(PDAC)手术中已成为一种常见的手术方式。一些研究描述了使用镰状韧带(FL)进行 MPV 重建,并取得了令人鼓舞的初步效果。
本研究旨在探讨与其他方法相比,该技术的可行性和疗效。
回顾性分析 2009 年至 2018 年间接受胰十二指肠切除术(PD)并伴有 MPV 切除术的 PDAC 患者的病历资料。区分并比较使用 FL 进行的 MPV 重建与其他技术。
146 例患者行 MPV 重建,其中 13 例行 FL 静脉成形术。其他重建技术包括直接端端吻合术(原发性,n=30)、侧静脉吻合术(LV,n=19)、聚四氟乙烯导管桥接术(PTFE,n=24)、髂动脉(IA)同种异体移植桥接术(n=47)和门静脉(PV)同种异体移植桥接术(n=13)。FL 组具有手术时间最短(p=0.023)、出血量最少(p=0.109)和术后住院时间最短(p=0.125)的优势。FL、原发性、LV、PTFE、IA 和 PV 的通畅率分别为 100%、90%、68%、54%、68%和 85%。组间比较显示,FL 具有最高的通畅率(p=0.008)和最低的抗血小板/抗凝比例(p=0.000)。不同技术的并发症和长期生存率相似。通畅组的中位生存时间(24.0 个月,95%CI:22.0-26.0)明显长于血栓形成组(17.0 个月,95%CI:13.7-20.3),但差异无统计学意义(P=0.148)。
PD 伴有 MPV 切除和重建,FL 是安全、可行和有效的,可能为患者带来潜在的益处。