From the Department of Anesthesiology and Critical Care Medicine, Peking University First Hospital, Beijing, China (XL, Z-ZX, Y-TL, Z-ML, Z-YL, D-XW) and Outcomes Research Consortium, Cleveland, Ohio, USA (D-XW).
Eur J Anaesthesiol. 2021 Mar 1;38(3):265-274. doi: 10.1097/EJA.0000000000001433.
Moderate-to-severe pain exists in the early postoperative period after laparoscopic renal surgery.
We investigated the analgesic effect of quadratus lumborum block (QLB) via two approaches in patients undergoing laparoscopic renal nephrectomy.
A randomised controlled trial.
An academic tertiary care hospital in Beijing, China.
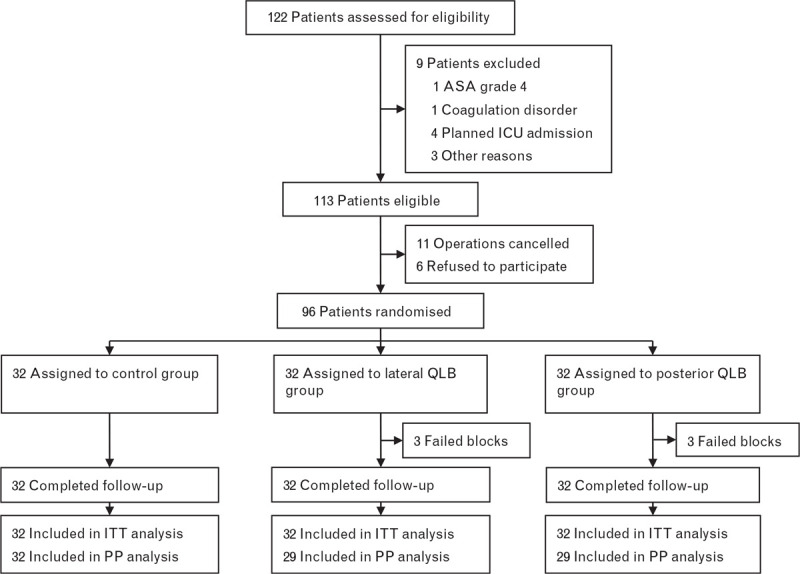
Ninety-six patients aged 18 to 70 years who were scheduled for elective laparoscopic radical or partial nephrectomy.
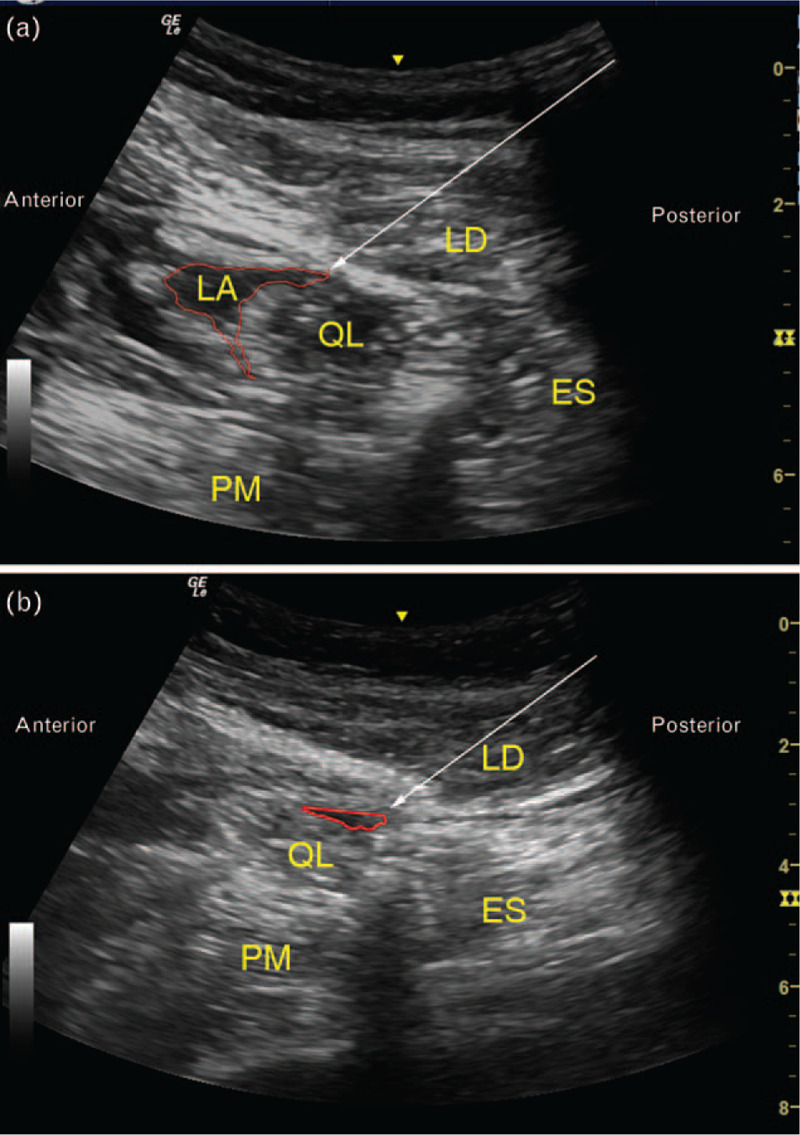
Eligible patients were allocated randomly to a control group (no block), lateral QLB group or posterior QLB group. Ultrasound-guided QLB was performed via either the lateral or posterior approach with 30 ml of 0.4% ropivacaine before surgery.
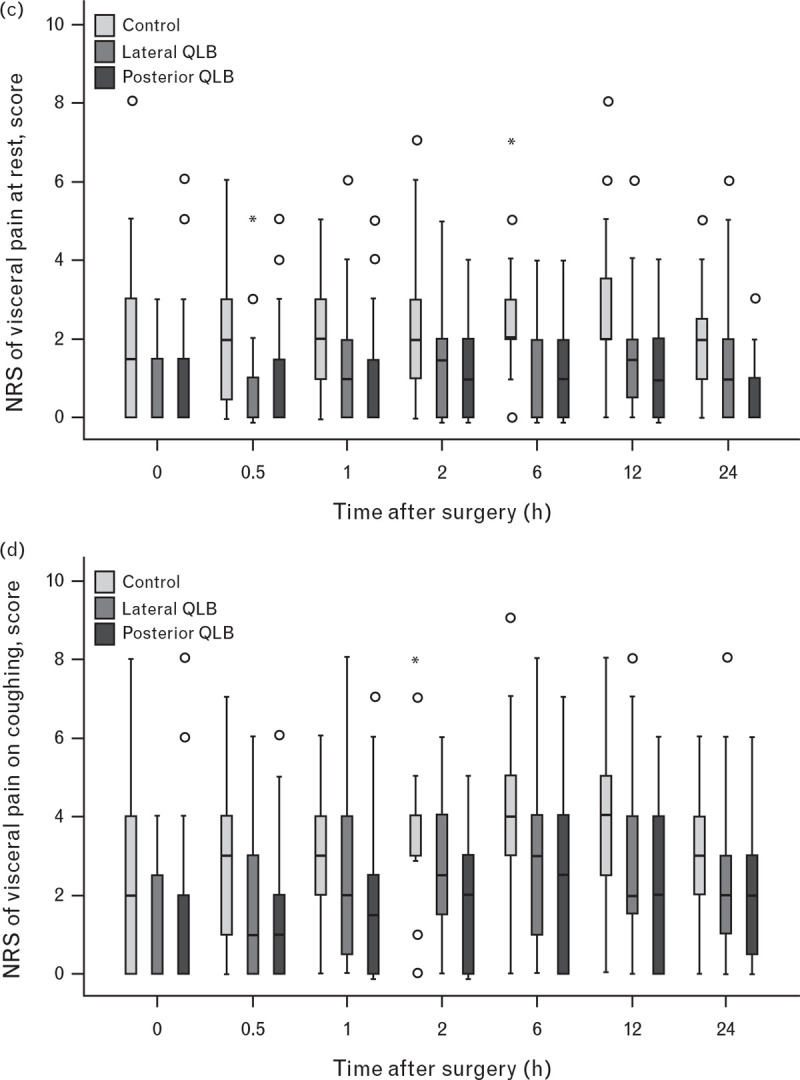
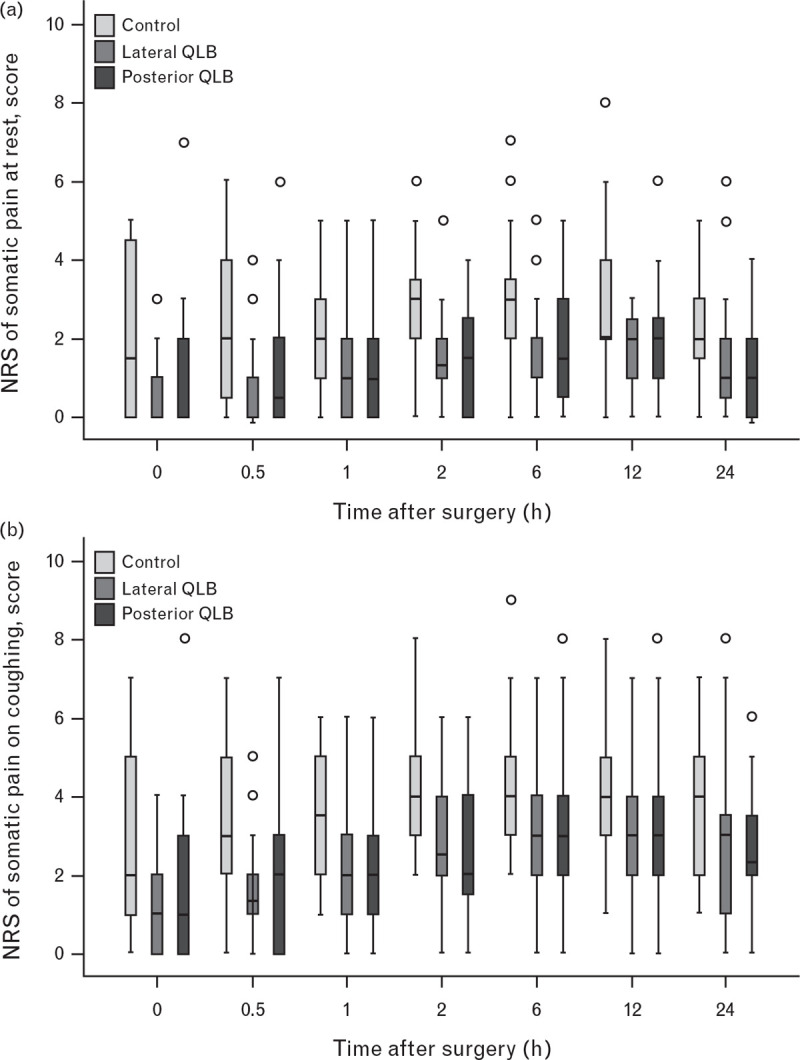
The primary outcome was sufentanil equivalent consumption within 24 h. Among secondary outcomes, somatic and visceral pain intensity at rest and on coughing were assessed with a numerical rating scale (where 0 = no pain and 10 = the worst pain) until 24 h postoperatively.
Sufentanil equivalent consumption did not differ among the three groups (118 ± 36 μg in the control group, 115 ± 47 μg in the lateral QLB group and 119 ± 40 μg in the posterior QLB group; P = 0.955). However, both somatic (lateral QLB vs. control, median difference -1, P < 0.001 at rest and -2 to -1, P < 0.001 on coughing; posterior QLB vs. control, -1, P < 0.001 at rest and -2 to -1, P < 0.001 on coughing) and visceral pain scores (lateral QLB vs. control, -1 to 0, P < 0.001 at rest and -1, P < 0.001 on coughing; posterior QLB vs. control, -1 to 0, P < 0.001 at rest and -2 to -1, P < 0.001 on coughing) were significantly lower in the two QLB groups than in the control group.
For patients undergoing laparoscopic renal surgery, a pre-operative single-shot QLB via the lateral or posterior approach did not decrease opioid consumption, but improved analgesia for up to 24 h after surgery.
www.chictr.org.cn identifier: ChiCTR1800019883.
腹腔镜肾手术后的早期会出现中重度疼痛。
我们研究了经两种入路行腰方肌阻滞(QLB)对腹腔镜肾切除术患者的镇痛效果。
随机对照试验。
中国北京一家学术性三级护理医院。
96 名年龄在 18 至 70 岁之间的择期行腹腔镜根治性或部分肾切除术的患者。
符合条件的患者被随机分配到对照组(无阻滞)、侧 QLB 组或后 QLB 组。手术前,通过超声引导行 QLB,用 0.4%罗哌卡因 30ml 分别从前外侧或后外侧入路进行阻滞。
主要观察指标是术后 24 小时内舒芬太尼等效消耗量。次要观察指标为术后 24 小时内静息和咳嗽时躯体和内脏疼痛强度,采用数字评分量表(0=无痛,10=最痛)评估。
三组舒芬太尼等效消耗量无差异(对照组 118±36μg,侧 QLB 组 115±47μg,后 QLB 组 119±40μg;P=0.955)。然而,躯体痛(侧 QLB 组与对照组相比,静息时差值-1,P<0.001;咳嗽时差值-2 至-1,P<0.001;后 QLB 组与对照组相比,静息时差值-1,P<0.001;咳嗽时差值-2 至-1,P<0.001)和内脏痛评分(侧 QLB 组与对照组相比,静息时差值-1 至 0,P<0.001;咳嗽时差值-1,P<0.001;后 QLB 组与对照组相比,静息时差值-1 至 0,P<0.001;咳嗽时差值-2 至-1,P<0.001)均显著低于对照组。
对于行腹腔镜肾手术的患者,术前单次行腰方肌阻滞(经前外侧或后外侧入路)并不能减少阿片类药物的消耗,但可改善术后 24 小时内的镇痛效果。
www.chictr.org.cn 标识符:ChiCTR1800019883。