Joint Department of Biomedical Engineering, University of North Carolina and North Carolina State University, Chapel Hill, North Carolina, USA.
Division of Cardiovascular Medicine, Brigham and Women's Hospital, Boston, Massachusetts, USA.
J Am Geriatr Soc. 2021 May;69(5):1309-1318. doi: 10.1111/jgs.17004. Epub 2021 Jan 5.
BACKGROUND/OBJECTIVES: Obesity increases with age, is disproportionately prevalent in black populations, and is associated with heart failure with preserved ejection fraction (HFpEF). An "obesity paradox," or improved survival with obesity, has been reported in patients with HFpEF. The aim of this study was to examine whether racial differences exist in the temporal trends and outcomes associated with obesity among older patients with HFpEF.
Community surveillance of acute decompensated heart failure (ADHF) hospitalizations, sampled by stratified design from 2005 to 2014.
Atherosclerosis Risk in Communities Study (NC, MS, MD, MN).
A total of 10,147 weighted hospitalizations for ADHF (64% female, 74% white, mean age 77 years), with ejection fraction ≥50%.
ADHF classified by physician review, HFpEF defined by ejection fraction ≥50%. Body mass index (BMI) calculated from weight at hospital discharge. Obesity defined by BMI ≥30 kg/m , class III obesity by BMI ≥40 kg/m .
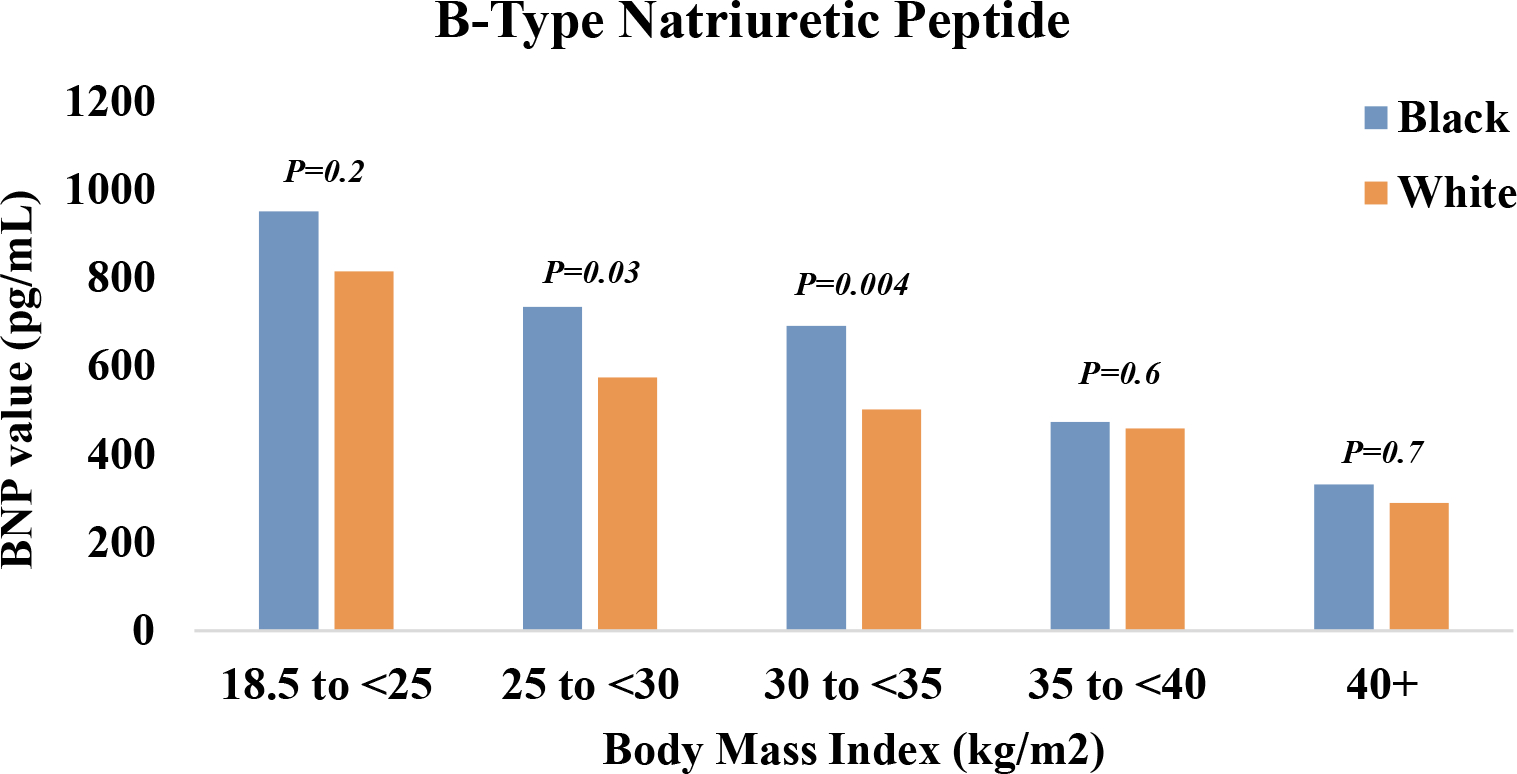
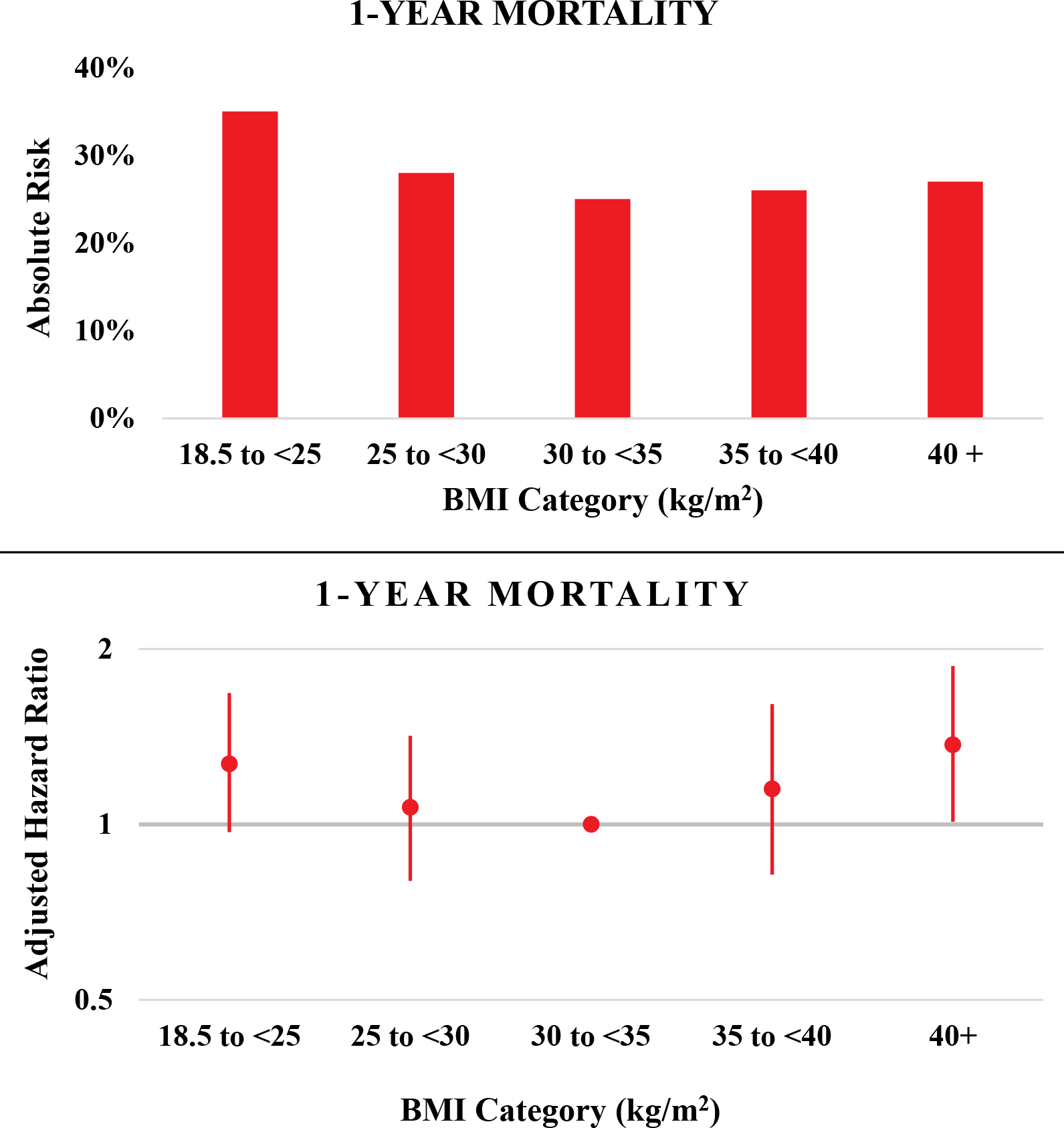
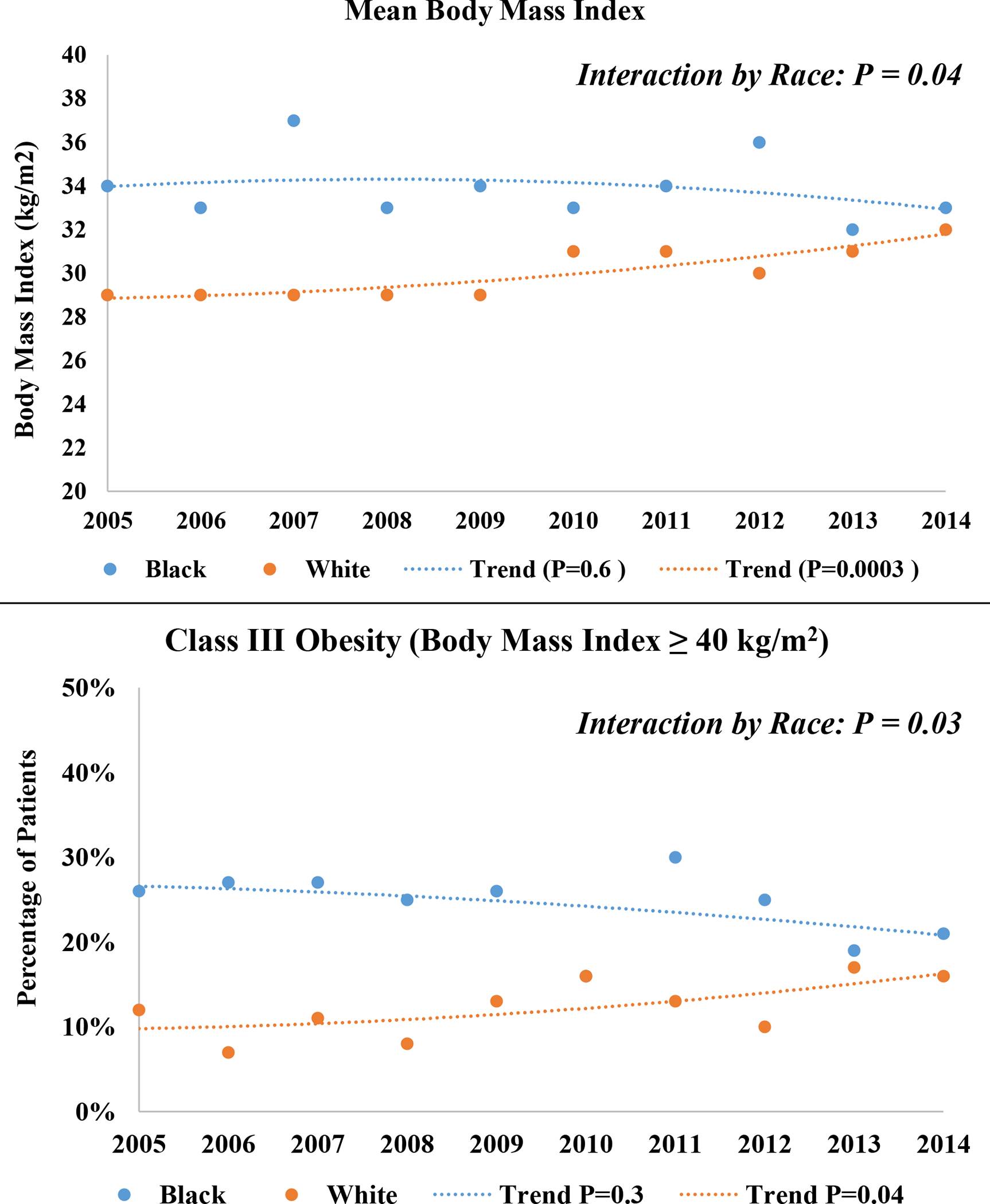
When aggregated across 2005-2014, the mean BMI was higher for black compared to white patients (34 vs 30 kg/m ; P < .0001), as was prevalence of obesity (56% vs 43%; P < .0001) and class III obesity (24% vs 13%; P < .0001). Over time, the annual mean BMI and prevalence of class III obesity remained stable for black patients, but steadily increased for white patients, with annual rates statistically differing by race (P-interaction = .04 and P = .03, respectively). For both races, a U-shaped adjusted mortality risk was observed across BMI categories, with the highest risk among patients with a BMI ≥40 kg/m .
Black patients were disproportionately burdened by obesity in this decade-long community surveillance of older hospitalized patients with HFpEF. However, temporal increases in mean BMI and class III obesity prevalence among white patients narrowed the racial difference in recent years. For both races, the worst survival was observed with class III obesity. Effective strategies are needed to manage obesity in patients with HFpEF.
背景/目的:肥胖随着年龄的增长而增加,在黑人群体中比例过高,与射血分数保留的心力衰竭(HFpEF)有关。在 HFpEF 患者中,已经报道了一种“肥胖悖论”,即肥胖与存活率提高有关。本研究旨在探讨在 HFpEF 老年患者中,肥胖与时间趋势和结局是否存在种族差异。
通过分层设计,从 2005 年到 2014 年对急性失代偿性心力衰竭(ADHF)住院患者进行社区监测。
动脉粥样硬化风险社区研究(北卡罗来纳州、密西西比州、马里兰州、明尼苏达州)。
共纳入 10147 例 ADHF 住院患者(64%为女性,74%为白人,平均年龄 77 岁),射血分数≥50%。
ADHF 由医生评估,HFpEF 定义为射血分数≥50%。体重指数(BMI)由出院时体重计算得出。BMI≥30kg/m 定义为肥胖,BMI≥40kg/m 定义为肥胖症 3 级。
2005-2014 年,黑人患者的平均 BMI 高于白人患者(34 比 30kg/m;P<.0001),肥胖的患病率(56%比 43%;P<.0001)和肥胖症 3 级(24%比 13%;P<.0001)也较高。随着时间的推移,黑人患者的年度平均 BMI 和肥胖症 3 级的患病率保持稳定,但白人患者的 BMI 和肥胖症 3 级的患病率稳步上升,种族之间的年度差异具有统计学意义(P 交互作用=.04,P=.03)。对于两种种族,BMI 类别与调整后的死亡率呈 U 形相关,BMI≥40kg/m 的患者风险最高。
在这项对 HFpEF 老年住院患者长达十年的社区监测中,黑人患者肥胖问题的负担不成比例。然而,近年来,白人患者平均 BMI 和肥胖症 3 级患病率的增加缩小了种族差异。对于两种种族,肥胖症 3 级的患者存活率最差。需要有效的策略来管理 HFpEF 患者的肥胖问题。