Tsuji Shigetsugu, Doyama Hisashi, Tsuyama Sho, Dejima Akihiro, Nakashima Takashi, Wakita Shigenori, Kito Yosuke, Nakanishi Hiroyoshi, Yoshida Naohiro, Katayanagi Kazuyoshi, Minato Hiroshi, Yao Takashi, Yao Kenshi
Department of Gastroenterology, Ishikawa Prefectural Central Hospital, Kanazawa, Japan.
Department of Human Pathology, Graduate School of Medicine, Juntendo University, Tokyo, Japan.
Endosc Int Open. 2021 Jan;9(1):E58-E65. doi: 10.1055/a-1293-7487. Epub 2021 Jan 1.
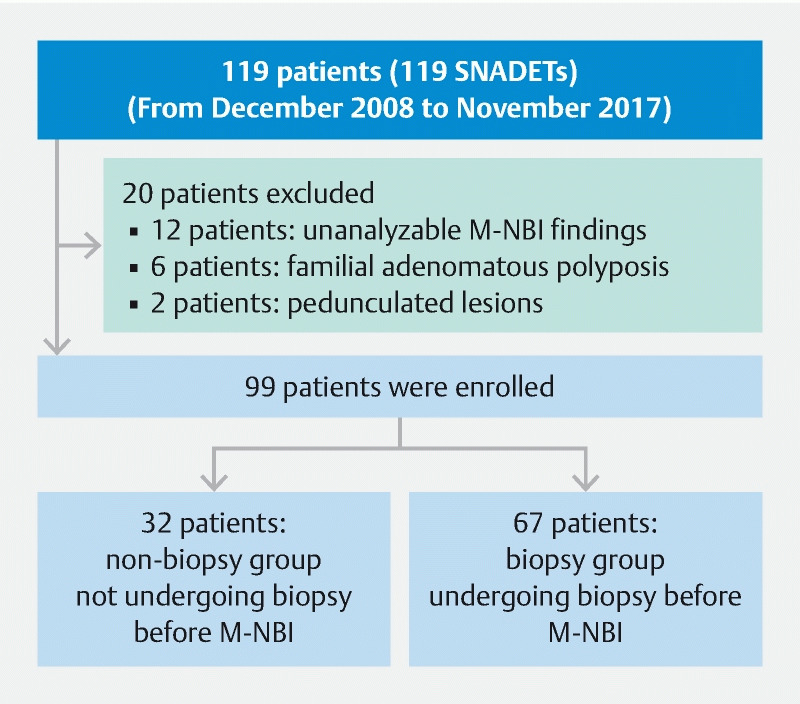
We aimed to evaluate the diagnostic performance of magnifying endoscopy with narrow-band imaging (M-NBI) in superficial non-ampullary duodenal epithelial tumors (SNADETs) regarding the absence or presence of biopsy before M-NBI diagnosis. Clinicopathological data were retrospectively reviewed for 99 SNADETs from 99 patients who underwent endoscopic resection. The 99 tumors were divided into the non-biopsy group (32 lesions not undergoing biopsy before M-NBI examination) and the biopsy group (67 lesions undergoing biopsy before M-NBI examination). We investigated the correlation between the M-NBI diagnosis and the histopathological diagnosis of the SNADETs in both groups. According to the modified revised Vienna classification, 31 tumors were classified as category 3 (C3) (low-grade adenoma) and 68 as category 4/5 (C4/5) (high-grade adenoma/cancer). The accuracy, sensitivity, and specificity of preoperative M-NBI diagnoses in the non-biopsy group vs the biopsy group were 88 % (95 % confidence interval: 71.0 - 96.5) vs 66 % (51.5 - 75.5), = 0.02; 95 % (77.2 - 99.9) vs 89 % (76.4 - 96.4), = 0.39; and 70 % (34.8 - 93.3) vs 14 % (3.0 - 36.3), < 0.01, respectively. Notably, in the biopsy group, the specificity of M-NBI in SNADETs was low at only 14 % because we over-diagnosed most C3 lesions as C4/5. M-NBI findings might have been compromised by the previous biopsy procedure itself. In the non-biopsy group, the accuracy of M-NBI in SNADETs was excellent in distinguishing C4/5 lesions from C3. The M-NBI findings in SNADETs should be evaluated while carefully considering the influence of a previous biopsy.
我们旨在评估窄带成像放大内镜(M-NBI)在浅表非壶腹十二指肠上皮肿瘤(SNADETs)中的诊断性能,同时考虑M-NBI诊断前是否进行活检。对99例行内镜切除的患者的99个SNADETs的临床病理数据进行回顾性分析。99个肿瘤分为未活检组(32个病变在M-NBI检查前未进行活检)和活检组(67个病变在M-NBI检查前进行了活检)。我们研究了两组中SNADETs的M-NBI诊断与组织病理学诊断之间的相关性。根据改良的维也纳分类,31个肿瘤被分类为3类(C3)(低级别腺瘤),68个被分类为4/5类(C4/5)(高级别腺瘤/癌)。未活检组与活检组术前M-NBI诊断的准确性、敏感性和特异性分别为88%(95%置信区间:71.0 - 96.5)对66%(51.5 - 75.5),P = 0.02;95%(77.2 - 99.9)对89%(76.4 - 96.4),P = 0.39;70%(34.8 - 93.3)对14%(3.0 - 36.3),P < 0.01。值得注意的是,在活检组中,M-NBI对SNADETs的特异性仅为14%,较低级别,因为我们将大多数C3病变过度诊断为C4/5。先前的活检操作本身可能影响了M-NBI的检查结果。在未活检组中,M-NBI在区分SNADETs的C4/5病变与C3病变方面准确性极佳。在评估SNADETs的M-NBI检查结果时,应仔细考虑先前活检的影响。