Chu Sherman S, White Heather O, Rindone Shannon L, Tripp Susan A, Rhein Lawrence M
Department of Pediatrics, University of Massachusetts Memorial Medical Center, Worcester, Mass.
Pediatr Qual Saf. 2020 Dec 28;6(1):e366. doi: 10.1097/pq9.0000000000000366. eCollection 2021 Jan-Feb.
Very low birth weight infants often demonstrate poor postnatal longitudinal growth, which negatively impacts survival rates and long-term health outcomes. Improving extrauterine growth restriction (EUGR) among extremely premature infants has become a significant focus of quality improvement initiatives. Prior efforts in the University of Massachusetts Memorial Medical Center neonatal intensive care unit were unsuccessful in improving the EUGR rate at discharge.
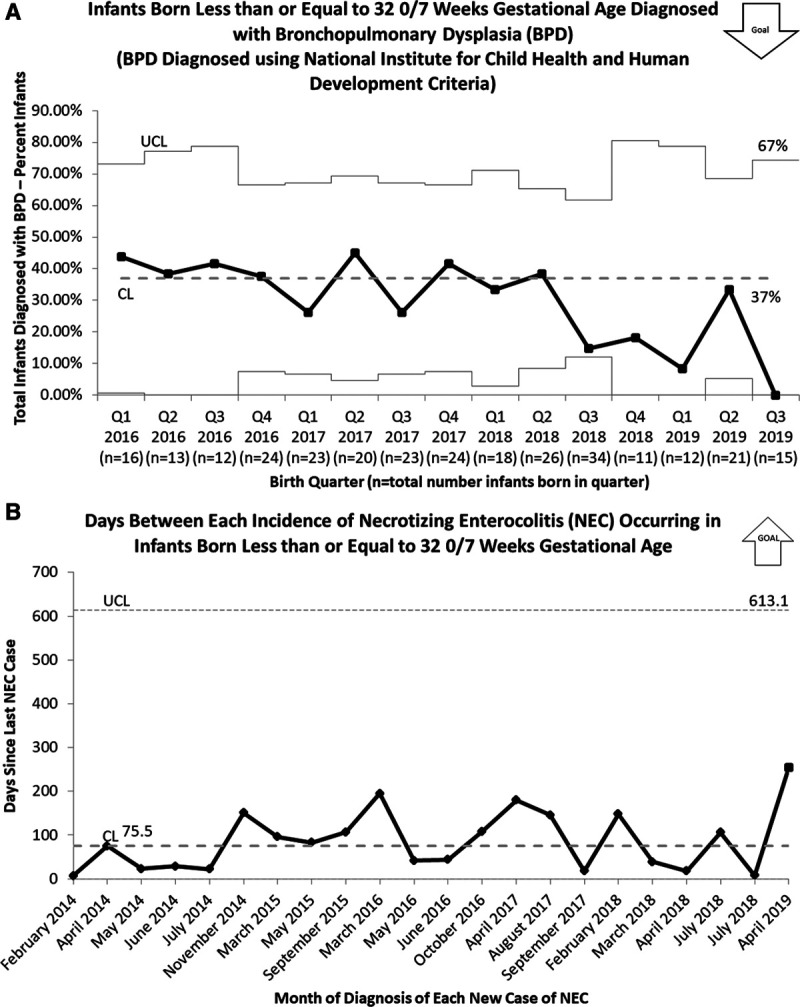
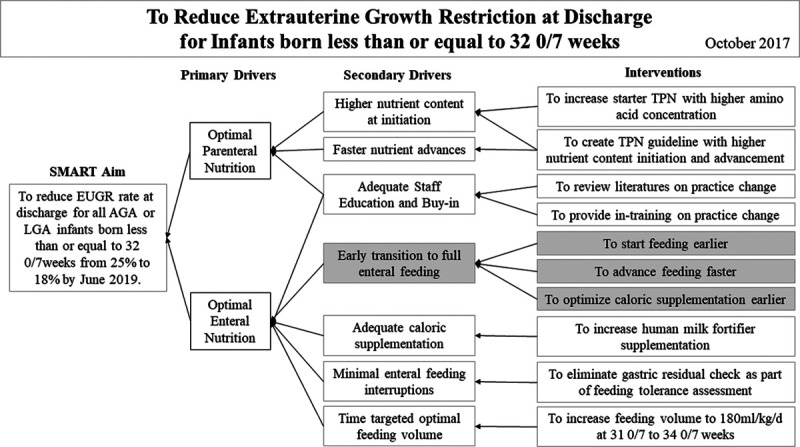
The primary aim of this initiative was to improve EUGR at discharge [defined as weight less than 10th percentile for postmenstrual age (PMA)] for infants born ≤32 0/7 weeks from a baseline of 25% to 20% by June 2019. We excluded all small for gestational age infants due to the limitation in the EUGR definition. A multidisciplinary team implemented evidence-based nutritional guideline changes using the Institute of Healthcare Improvement methods. The most notable change was the time-specific feeding volume advancement that increased the goal feeding volume between 31 0/7 and 34 0/7 weeks PMA from 150-160 to 170-180 milliliters per kilogram per day. The team monitored nutritional intake, weight, necrotizing enterocolitis (NEC), bronchopulmonary dysplasia (BPD), and length of stay (LOS).
The EUGR rate improved from 25% to 12% after initiation of increased time-specific, enteral feeding guidelines at 31-34 weeks PMA. NEC rate, BPD rate, and LOS remained unchanged throughout the initiative.
By implementing a time-specific volume increase guideline from 31 0/7 to 34 0/7 weeks PMA, the EUGR rate improved from baseline of 25% to 12% without increasing NEC rate, BPD rate, and LOS.
极低出生体重儿通常出生后纵向生长不佳,这对存活率和长期健康结局产生负面影响。改善极早早产儿宫外生长受限(EUGR)已成为质量改进举措的重要关注点。此前马萨诸塞大学纪念医学中心新生儿重症监护病房在改善出院时的EUGR发生率方面未取得成功。
该举措的主要目标是将出生孕周≤32⁰/₇周的婴儿出院时的EUGR(定义为出生后胎龄体重低于第10百分位数)从基线的25%降至2019年6月时的20%。由于EUGR定义的限制,我们排除了所有小于胎龄儿。一个多学科团队采用医疗保健改进研究所的方法实施了基于证据的营养指南变更。最显著的变更是特定时间的喂养量增加,即出生后胎龄31⁰/₇至34⁰/₇周时目标喂养量从每天每千克150 - 160毫升增加至170 - 180毫升。该团队监测了营养摄入量、体重、坏死性小肠结肠炎(NEC)、支气管肺发育不良(BPD)以及住院时长(LOS)。
在出生后胎龄31 - 34周实施增加特定时间肠内喂养指南后,EUGR发生率从25%降至12%。在整个举措实施过程中,NEC发生率、BPD发生率和住院时长保持不变。
通过实施出生后胎龄31⁰/₇至34⁰/₇周特定时间的喂养量增加指南,EUGR发生率从基线的25%降至12%,且未增加NEC发生率、BPD发生率和住院时长。