Vadu Rural Health Program, King Edward Memorial Hospital Research Centre (KEMHRC), Rasta Peth, Pune, Maharashtra, 411011, India.
Symbiosis Institute of Health Sciences, Symbiosis International (Deemed) University, Lavale, Mulshi, Pune, Maharashtra, 411011, India.
Hum Resour Health. 2021 Jan 6;19(1):7. doi: 10.1186/s12960-020-00546-z.
Globally, community health workers (CHWs) are integral contributors to many health systems. In India, Accredited Social Health Activists (ASHAs) have been deployed since 2005. Engaged in multiple health care activities, they are a key link between the health system and population. ASHAs are expected to participate in new health programmes prompting interest in their current workload from the perspective of the health system, community and their family.
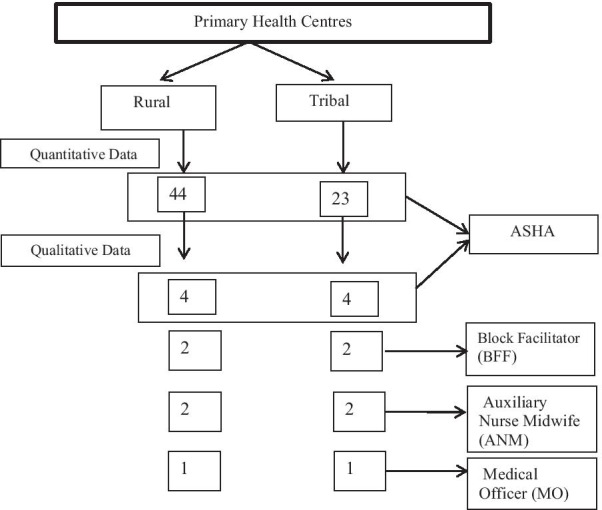
This mixed-methods design study was conducted in rural and tribal Primary Health Centers (PHCs), in Pune district, Western Maharashtra, India. All ASHAs affiliated with these PHCs were invited to participate in the quantitative study, those agreeing to contribute in-depth interviews (IDI) were enrolled in an additional qualitative study. Key informants' interviews were conducted with the Auxiliary Nurse Midwife (ANM), Block Facilitators (BFF) and Medical Officers (MO) of the same PHCs. Quantitative data were analysed using descriptive statistics. Qualitative data were analysed thematically.
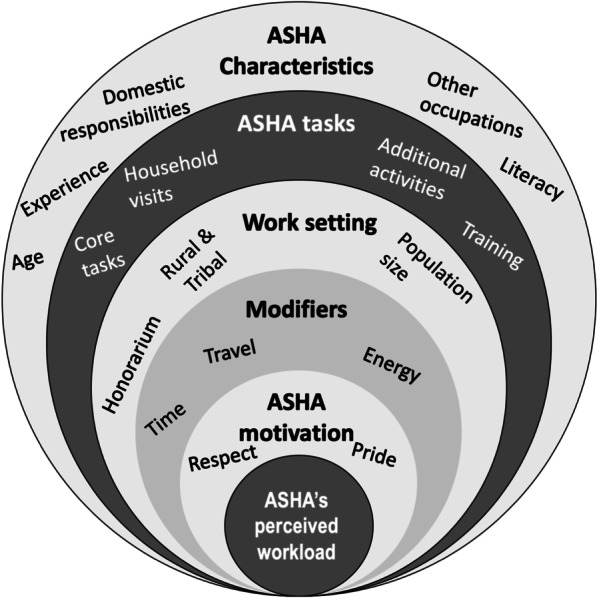
We recruited 67 ASHAs from the two PHCs. ASHAs worked up to 20 h/week in their village of residence, serving populations of approximately 800-1200, embracing an increasing range of activities, despite a workload that contributed to feelings of being rushed and tiredness. They juggled household work, other paid jobs and their ASHA activities. Practical problems with travel added to time involved, especially in tribal areas where transport is lacking. Their sense of benefiting the community coupled with respect and recognition gained in village brought happiness and job satisfaction. They were willing to take on new tasks. ASHAs perceived themselves as 'voluntary community health workers' rather than as 'health activists".
ASHAs were struggling to balance their significant ASHA work and domestic tasks. They were proud of their role as CHWs and willing to take on new activities. Strategies to recruit, train, skills enhancement, incentivise, and retain ASHAs, need to be prioritised. Evolving attitudes to the advantages/disadvantages of current voluntary status and role of ASHAs need to be understood and addressed if ASHAs are to be remain a key component in achieving universal health coverage in India.
在全球范围内,社区卫生工作者(CHW)是许多卫生系统的重要组成部分。在印度,自 2005 年以来,已部署了认证社会卫生活动家(ASHA)。从事多项医疗保健活动,他们是卫生系统与人口之间的重要纽带。预计 ASHA 将参与新的卫生计划,这促使人们从卫生系统、社区和家庭的角度关注他们目前的工作量。
这项混合方法设计研究在印度马哈拉施特拉邦浦那地区的农村和部落初级保健中心(PHC)进行。邀请所有隶属于这些 PHC 的 ASHA 参加定量研究,同意进行深入访谈(IDI)的人则参加额外的定性研究。对同一 PHC 的辅助护士助产士(ANM)、街区推动者(BFF)和医疗官进行了关键知情人访谈。使用描述性统计对定量数据进行分析。定性数据进行了主题分析。
我们从两个 PHC 招募了 67 名 ASHA。ASHA 在他们居住的村庄每周工作 20 小时,为大约 800-1200 人提供服务,尽管工作量很大,但他们还是承担了越来越多的活动,这导致他们感到匆忙和疲倦。他们兼顾家庭工作、其他有偿工作和 ASHA 活动。旅行中的实际问题增加了时间投入,特别是在缺乏交通的部落地区。他们觉得自己为社区带来了好处,并且在村里获得了尊重和认可,这给他们带来了快乐和工作满意度。他们愿意承担新的任务。ASHA 认为自己是“志愿社区卫生工作者”,而不是“卫生活动家”。
ASHA 正在努力平衡他们重要的 ASHA 工作和家庭任务。他们为自己作为 CHW 的角色感到自豪,并愿意承担新的活动。需要优先考虑招聘、培训、技能提升、激励和留住 ASHA 的策略。如果 ASHA 要继续成为印度实现全民健康覆盖的关键组成部分,就需要了解并解决当前自愿身份和 ASHA 角色的利弊的态度演变。