SingHealth Polyclinics, SingHealth, 167, Jalan Bukit Merah, Connection One, Tower 5, #15-10, Singapore, P.O. 150167, Singapore.
Institute of Data Science, National University of Singapore, Singapore, Singapore.
Lipids Health Dis. 2021 Jan 6;20(1):2. doi: 10.1186/s12944-020-01427-z.
Clinical trials have demonstrated that either initiating or up-titrating a statin dose substantially reduce Low-Density Lipoprotein-Cholesterol (LDL-C) levels. However, statin adherence in actual practice tends to be suboptimal, leading to diminished effectiveness. This study aims to use real-world data to determine the effect on LDL-C levels and LDL-C goal attainment rates, when selected statins are titrated in Asian patients.
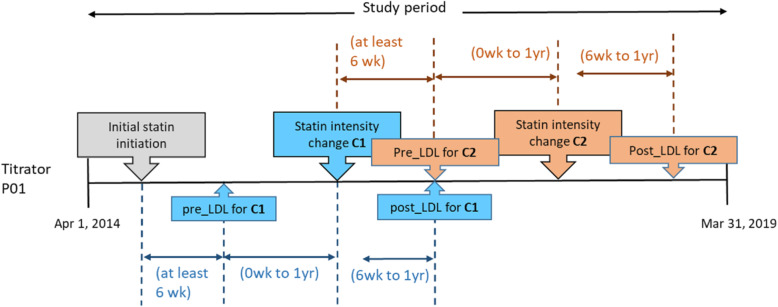
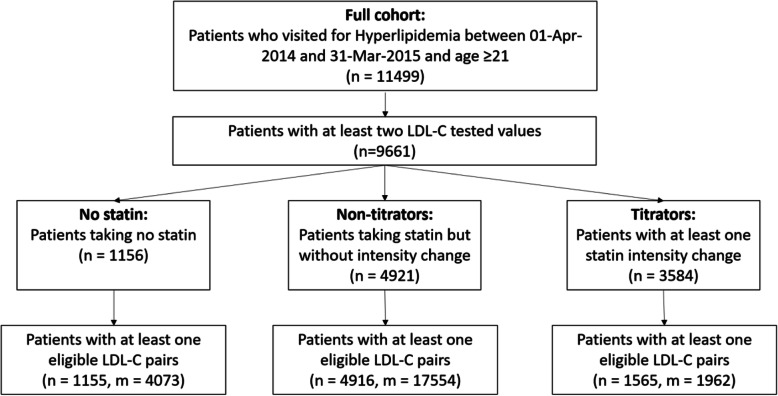
A retrospective cohort study over a 5-year period, from April 2014 to March 2019 was conducted on a cohort of multi-ethnic adult Asian patients with clinical diagnosis of Dyslipidaemia in a primary care clinic in Singapore. The statins were classified into low-intensity (LI), moderate-intensity (MI) and high-intensity (HI) groups according to the 2018 American College of Cardiology and American Heart Association (ACC/AHA) Blood Cholesterol Guidelines. Patients were grouped into "No statin", "Non-titrators" and "Titrators" cohorts based on prescribing patterns. For the "Titrators" cohort, the mean percentage change in LDL-C and absolute change in LDL-C goal attainment rates were computed for each permutation of statin intensity titration.
Among the cohort of 11,499 patients, with a total of 266,762 visits, there were 1962 pairs of LDL-C values associated with a statin titration. Initiation of LI, MI and HI statin resulted in a lowering of LDL-C by 21.6% (95%CI = 18.9-24.3%), 28.9% (95%CI = 25.0-32.7%) and 25.2% (95%CI = 12.8-37.7%) respectively. These were comparatively lower than results from clinical trials (30 to 63%). The change of LDL-C levels due to up-titration, down-titration, and discontinuation were - 12.4% to - 28.9%, + 13.2% to + 24.6%, and + 18.1% to + 32.1% respectively. The improvement in LDL-C goal attainment ranged from 26.5% to 47.1% when statin intensity was up-titrated.
In this study based on real-world data of Asian patients in primary care, it was shown that although statin titration substantially affected LDL-C levels and LDL-C goal attainment rates, the magnitude was lower than results reported from clinical trials. These results should be taken into consideration and provide further insight to clinicians when making statin adjustment recommendations in order to achieve LDL-C targets in clinical practice, particularly for Asian populations.
临床试验已经证明,起始或增加他汀类药物剂量可显著降低低密度脂蛋白胆固醇(LDL-C)水平。然而,他汀类药物在实际应用中的依从性往往不理想,导致疗效降低。本研究旨在利用真实世界的数据,确定在亚洲患者中调整选定他汀类药物剂量对 LDL-C 水平和 LDL-C 达标率的影响。
这是一项回顾性队列研究,在新加坡一家基层医疗机构的多民族成年亚裔血脂异常患者队列中进行,研究时间为 2014 年 4 月至 2019 年 3 月,为期 5 年。根据 2018 年美国心脏病学会/美国心脏协会(ACC/AHA)血脂指南,他汀类药物被分为低强度(LI)、中强度(MI)和高强度(HI)组。根据处方模式,患者被分为“无他汀类药物”、“非调整者”和“调整者”队列。对于“调整者”队列,计算了他汀类药物强度调整的每种排列方式下 LDL-C 的平均百分比变化和 LDL-C 达标率的绝对变化。
在队列的 11499 名患者中,共进行了 266762 次就诊,有 1962 对 LDL-C 值与他汀类药物剂量调整相关。起始使用 LI、MI 和 HI 他汀类药物可分别降低 LDL-C 21.6%(95%CI=18.9-24.3%)、28.9%(95%CI=25.0-32.7%)和 25.2%(95%CI=12.8-37.7%)。这些结果明显低于临床试验结果(30%至 63%)。由于剂量增加、剂量减少和停药导致的 LDL-C 水平变化分别为-12.4%至-28.9%、+13.2%至+24.6%和+18.1%至+32.1%。当他汀类药物强度上调时,LDL-C 达标率的改善范围为 26.5%至 47.1%。
本研究基于基层医疗机构亚裔患者的真实世界数据,表明尽管他汀类药物剂量调整对 LDL-C 水平和 LDL-C 达标率有显著影响,但幅度低于临床试验报告的结果。在临床实践中为达到 LDL-C 目标而调整他汀类药物时,临床医生应考虑这些结果并提供进一步的见解,特别是对于亚洲人群。