Department of Radiation Oncology, University Hospital Zürich, Rämistrasse 100, 8091, Zürich, Switzerland.
Department of Radiation Oncology, Marienhospital Stuttgart, Böheimstrasse 37, 70199, Stuttgart, Germany.
Radiat Oncol. 2021 Jan 6;16(1):4. doi: 10.1186/s13014-020-01730-0.
Metastasis directed treatment (MDT) is increasingly performed with the attempt to improve outcome in non-small cell lung cancer (NSCLC) patients receiving targeted- or immunotherapy (TT/IT). This study aimed to assess the safety and efficacy of metastasis directed stereotactic radiotherapy (SRT) concurrent to TT/IT in NSCLC patients.
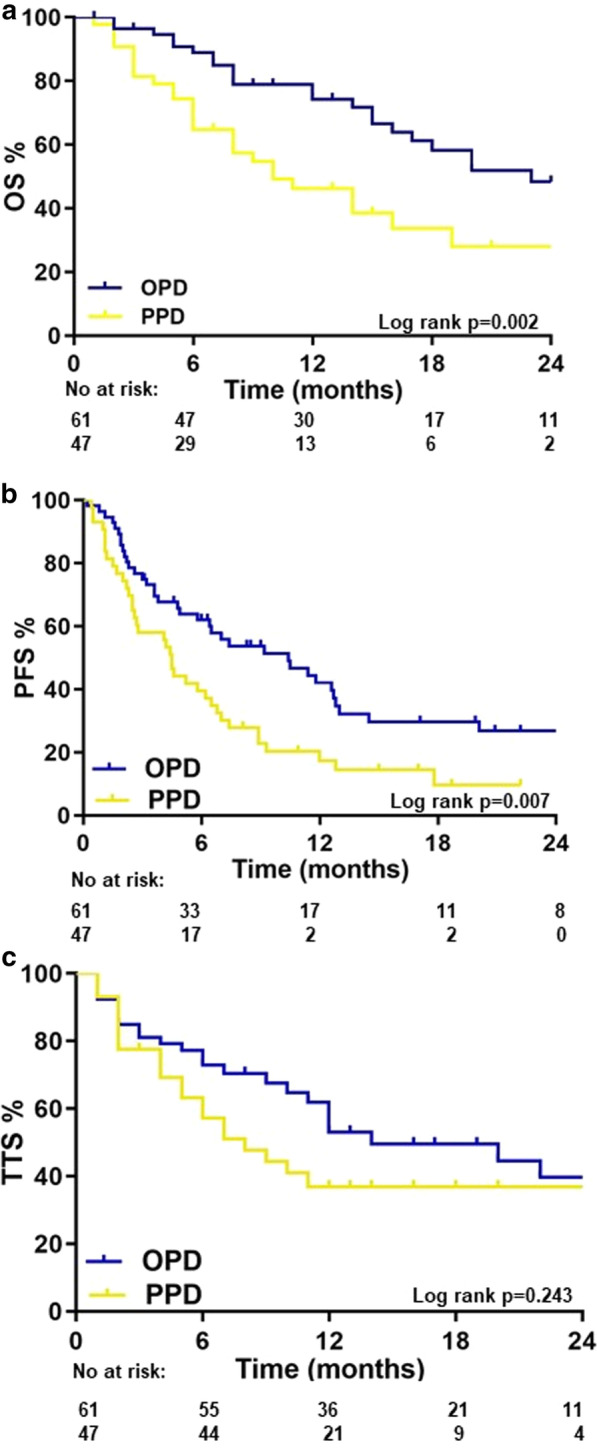
A retrospective multicenter cohort of stage IV NSCLC patients treated with TT/IT and concurrent (≤ 30 days) MDT was established. 56% and 44% of patients were treated for oligoprogressive disease (OPD) or polyprogressive disease (PPD) under TT/IT, polyprogressive respectively. Survival was analyzed using Kaplan-Meier and log rank testing. Toxicity was scored using CTCAE v4.03 criteria. Predictive factors for overall survival (OS), progression free survival (PFS) and time to therapy switch (TTS) were analyzed with uni- and multivariate analysis.
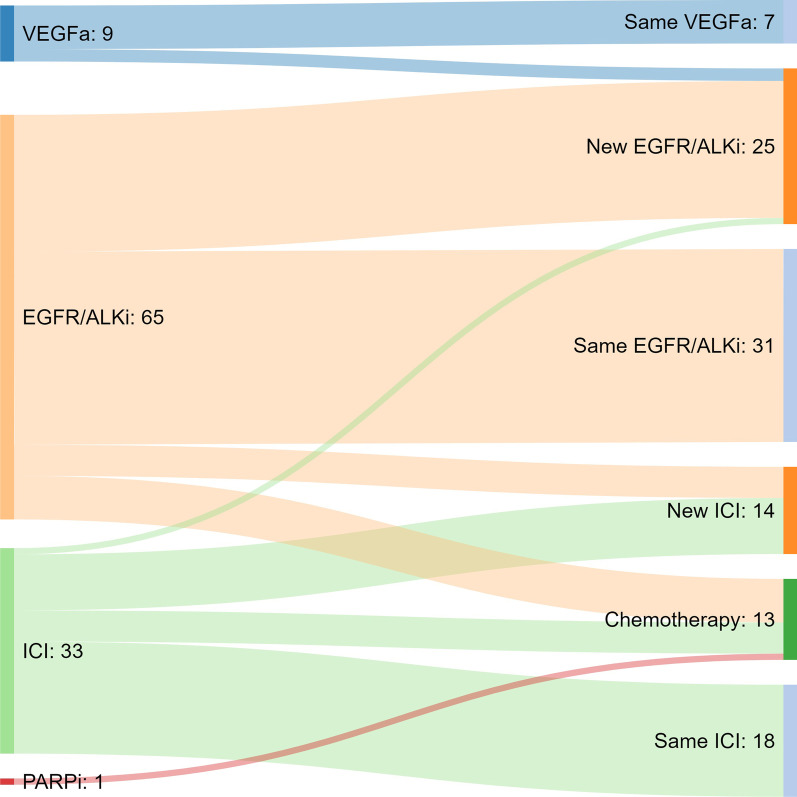
MDT of 192 lesions in 108 patients was performed between 07/2009 and 05/2018. Concurrent TT/IT consisted of EGFR/ALK-inhibitors (60%), immune checkpoint inhibitors (31%), VEGF-antibodies (8%) and PARP-inhibitors (1%). 2y-OS was 51% for OPD and 25% for PPD. After 1 year, 58% of OPD and 39% of PPD patients remained on the same TT/IT. Second progression after MDT was oligometastatic (≤ 5 lesions) in 59% of patients. Severe acute and late toxicity was observed in 5.5% and 1.9% of patients. In multivariate analysis, OS was influenced by the clinical metastatic status (p = 0.002, HR 2.03, 95% CI 1.30-3.17). PFS was better in patients receiving their first line of systemic treatment (p = 0.033, HR 1.7, 95% CI 1.05-2.77) and with only one metastases-affected organ (p = 0.023, HR 2.04, 95% CI 1.10-3.79). TTS was 6 months longer in patients with one metastases-affected organ (p = 0.031, HR 2.53, 95% CI 1.09-5.89). Death was never therapy-related.
Metastases-directed SRT in NSCLC patients can be safely performed concurrent to TT/IT with a low risk of severe toxicity. To find the ideal sequence of the available multidisciplinary treatment options for NSCLC and determine what patients will benefit most, a further evaluated in a broader context within prospective clinical trials is needed continuation of TT/IT beyond progression combined with MDT for progressive lesions appears promising but requires prospective evaluation.
retrospectively registered.
转移性疾病定向治疗(MDT)越来越多地用于尝试改善接受靶向或免疫治疗(TT/IT)的非小细胞肺癌(NSCLC)患者的预后。本研究旨在评估 NSCLC 患者在 TT/IT 治疗期间同时进行转移性疾病定向立体定向放疗(SRT)的安全性和有效性。
建立了一个回顾性多中心队列,纳入了接受 TT/IT 和同期(≤30 天)MDT 的 IV 期 NSCLC 患者。56%和 44%的患者分别接受 TT/IT 治疗以治疗寡进展性疾病(OPD)或多进展性疾病(PPD)。使用 Kaplan-Meier 和对数秩检验分析生存情况。使用 CTCAE v4.03 标准对毒性进行评分。使用单因素和多因素分析对总生存期(OS)、无进展生存期(PFS)和治疗转换时间(TTS)的预测因素进行分析。
在 2009 年 7 月至 2018 年 5 月期间,对 108 名患者的 192 个病灶进行了 MDT。同期 TT/IT 治疗包括 EGFR/ALK 抑制剂(60%)、免疫检查点抑制剂(31%)、VEGF 抗体(8%)和 PARP 抑制剂(1%)。OPD 的 2 年 OS 为 51%,PPD 为 25%。1 年后,OPD 中有 58%和 PPD 中有 39%的患者仍在接受相同的 TT/IT 治疗。MDT 后第二次进展为寡转移(≤5 个病灶)的患者占 59%。5.5%和 1.9%的患者出现严重急性和迟发性毒性。多因素分析显示,OS 受临床转移状态影响(p=0.002,HR 2.03,95%CI 1.30-3.17)。首次接受系统治疗的患者(p=0.033,HR 1.7,95%CI 1.05-2.77)和仅有一个转移受累器官的患者(p=0.023,HR 2.04,95%CI 1.10-3.79)的 PFS 更好。有一个转移受累器官的患者的 TTS 延长了 6 个月(p=0.031,HR 2.53,95%CI 1.09-5.89)。死亡从未与治疗相关。
在 TT/IT 治疗期间,对 NSCLC 患者进行转移性疾病定向 SRT 具有较低的严重毒性风险,是安全的。为了找到 NSCLC 患者现有多学科治疗方案的理想顺序,并确定哪些患者将受益最大,需要在更广泛的背景下进一步评估前瞻性临床试验中继续进行 TT/IT 治疗,以克服进展并结合 MDT 治疗进展性病变。