Department of Radiation Oncology, Fudan University Shanghai Cancer Center, 270 Dong An Road, Shanghai, 200032, China.
Department of Oncology, Shanghai Medical College, Fudan University, Shanghai, 200032, China.
Radiat Oncol. 2019 Mar 13;14(1):44. doi: 10.1186/s13014-019-1240-1.
Despite development of several next-generation tyrosine kinase inhibitors (TKIs), crizotinib remains one of the first-line treatment options for advanced ALK-positive NSCLC and is widely used in situations where next-generation TKIs aren't yet approved or economically inaccessible. However, the pattern of failure and clinical value of radiotherapy in metastatic crizotinib-treated ALK-mutant lung cancer, with or without baseline brain metastases (BBM), are largely unknown.
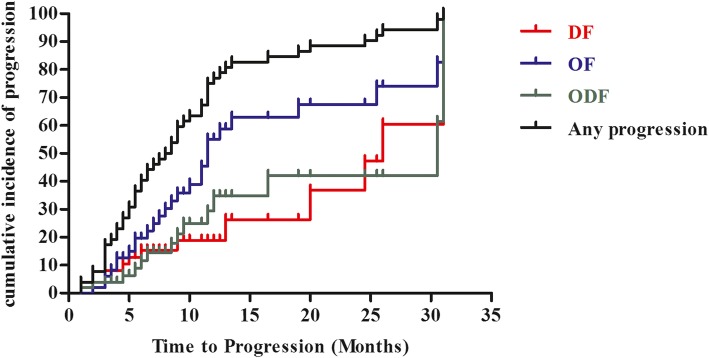
Consecutive crizotinib-treated NSCLC patients with adequate imaging and measurable disease were retrospectively enrolled. Disease progression in original sites (primary/metastatic), new sites, or both, are classified as original failure (OF), distant failure (DF) and ODF, respectively. Progression free survival, from crizotinib initiation to the first disease progression, and from that to the second disease progression, were calculated as PFS1 and PFS2.
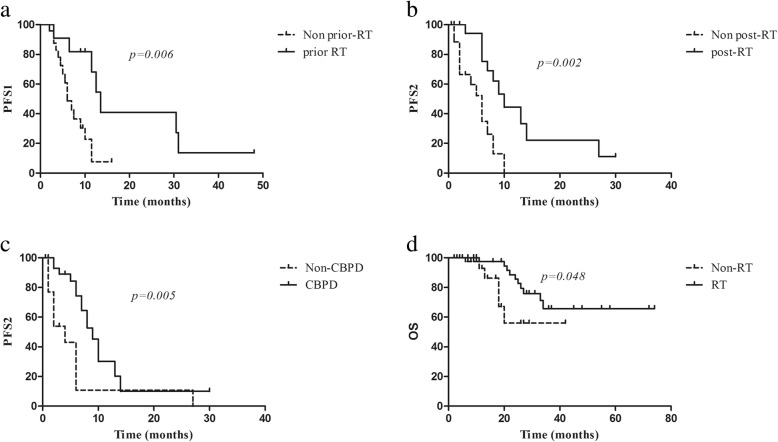
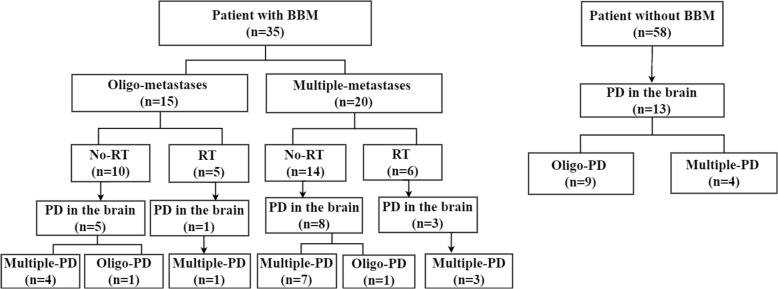
Ninety-three patients were identified. With a median follow up of 22.0 (range, 2.0-72.0) months, 52 patients had crizotinib-treatment failure. The frequencies of OF, ODF, and DF, were 50.0, 26.9, and 23.1%, respectively. Histology, primary tumor size and presence of BBM, were independently associated with OF, using competing risks analyses. The brain was the most common site of initial disease progression. Patients with BBM had a significant higher possibility developing multiple-progressive lesions in the brain (p = 0.002). Importantly, four of the ten patients who had baseline oligo-metastatic cranial disease but didn't receive upfront brain radiation, developed multiple-progressive disease in the brain. Brain radiation before crizotinib could alter the disease failure patterns and improve PFS1 among patients with BBM (p = 0.006). Extracranial radiation was efficient in controlling symptoms but it was not associated with PFS1 (p = 0.223), and the majority of patients were eligible for salvage radiotherapy upon disease progression to crizotinib. By the time of data cut-off, 28 patients had second disease progression, with a median PFS2 of 7.0 (95% CI 5.4-8.6) months and salvage radiotherapy significantly prolonged PFS2 (p = 0.003). Additionally, patients receiving any radiotherapy during their treatment course had a significant longer overall survival (p = 0.048).
Among patients with baseline oligo-metastatic brain lesions which are suitable for stereotactic radiosurgery, upfront brain radiotherapy provides considerable clinical benefits. While, extracranial radiation may be deferred in asymptomatic patients with multiple-metastatic lesions.
尽管已经开发出了几种下一代酪氨酸激酶抑制剂(TKI),但克唑替尼仍然是治疗晚期ALK 阳性 NSCLC 的一线治疗选择之一,并且在尚未批准或无法获得经济上的下一代 TKI 的情况下广泛使用。然而,在有或没有基线脑转移(BBM)的情况下,转移性克唑替尼治疗的 ALK 突变肺癌中,放疗的失败模式和临床价值在很大程度上是未知的。
回顾性纳入了连续接受克唑替尼治疗的 NSCLC 患者,这些患者有足够的影像学和可测量的疾病。原始部位(原发性/转移性)、新部位或两者的疾病进展分别归类为原发性失败(OF)、远处失败(DF)和 ODF。从克唑替尼开始到第一次疾病进展,以及从那时到第二次疾病进展的无进展生存期,分别计算为 PFS1 和 PFS2。
确定了 93 例患者。中位随访时间为 22.0(范围,2.0-72.0)个月,52 例患者发生了克唑替尼治疗失败。OF、ODF 和 DF 的频率分别为 50.0%、26.9%和 23.1%。使用竞争风险分析,组织学、原发肿瘤大小和 BBM 的存在与 OF 独立相关。大脑是最初疾病进展的最常见部位。有 BBM 的患者在脑内发生多个进展性病变的可能性显著更高(p=0.002)。重要的是,基线寡转移性颅疾病但未接受 upfront 脑放疗的 10 名患者中的 4 名在脑内发生了多个进展性疾病。在接受克唑替尼治疗之前进行脑放疗可以改变疾病的失败模式,并提高有 BBM 的患者的 PFS1(p=0.006)。颅外放疗可有效控制症状,但与 PFS1 无关(p=0.223),并且大多数患者在疾病进展至克唑替尼时都有资格接受挽救性放疗。截至数据截止日期,28 例患者发生了第二次疾病进展,中位 PFS2 为 7.0(95%CI 5.4-8.6)个月,挽救性放疗显著延长了 PFS2(p=0.003)。此外,在治疗过程中接受任何放疗的患者的总生存期显著延长(p=0.048)。
对于适合立体定向放疗的基线寡转移性脑病变患者, upfront 脑放疗提供了显著的临床获益。然而,对于有多个转移性病变且无症状的患者,可以推迟颅外放疗。