Toronto HHT Centre, Li Ka Shing Knowledge Institute, St. Michael's Hospital, 30 Bond St, Toronto, ON, M5B-1W8, USA.
Division of Respirology, Department of Medicine, University of Toronto, Toronto, Canada.
Orphanet J Rare Dis. 2021 Jan 6;16(1):12. doi: 10.1186/s13023-020-01579-2.
Retrospective questionnaire and healthcare administrative data suggest reduced life expectancy in untreated hereditary hemorrhagic telangiectasia (HHT). Prospective data suggests similar mortality, to the general population, in Denmark's centre-treated HHT patients. However, clinical phenotypes vary widely in HHT, likely affecting mortality. We aimed to measure predictors of mortality among centre-treated HHT patients. HHT patients were recruited at 14 HHT centres of the Brain Vascular Malformation Consortium (BVMC) since 2010 and followed annually. Vital status, organ vascular malformations (VMs) and clinical symptoms data were collected at baseline and during follow-up (N = 1286). We tested whether organ VMs, HHT symptoms and HHT genes were associated with increased mortality using Cox regression analysis, adjusting for patient age, sex, and smoking status.
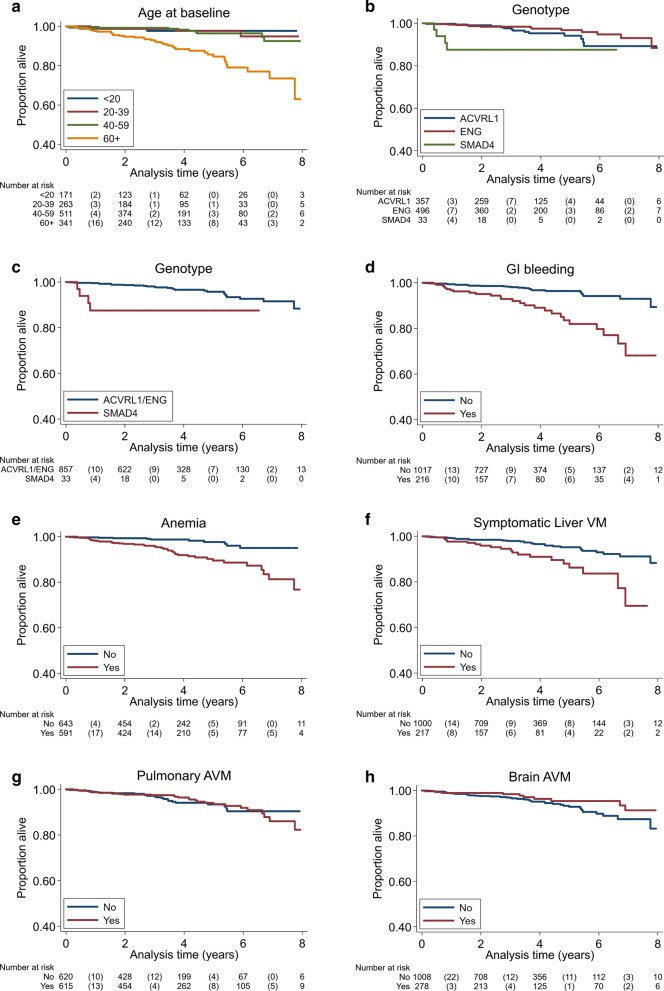
59 deaths occurred over average follow-up time of 3.4 years (max 8.6 years). A history of anemia was associated with increased mortality (HR = 2.93, 95% CI 1.37-6.26, p = 0.006), as were gastro-intestinal (GI) bleeding (HR = 2.63, 95% CI 1.46-4.74, p = 0.001), and symptomatic liver VMs (HR = 2.10, 95% CI 1.15-3.84, p = 0.015). Brain VMs and pulmonary arteriovenous malformations (AVMs) were not associated with mortality (p > 0.05). Patients with SMAD4 mutation had significantly higher mortality (HR = 18.36, 95% CI 5.60-60.20, p < 0.001) compared to patients with ACVRL1 or ENG mutation, but this estimate is imprecise given the rarity of SMAD4 patients (n = 33, 4 deaths).
Chronic GI bleeding, anemia and symptomatic liver VMs are associated with increased mortality in HHT patients, independent of age, and in keeping with the limited treatment options for these aspects of HHT. Conversely, mortality does not appear to be associated with pulmonary AVMs or brain VMs, for which patients are routinely screened and treated preventatively at HHT Centres. This demonstrates the need for development of new therapies to treat chronic anemia, GI bleeding, and symptomatic liver VMs in order to reduce mortality among HHT patients.
回顾性问卷调查和医疗保健管理数据表明,未经治疗的遗传性出血性毛细血管扩张症(HHT)患者的预期寿命会缩短。丹麦的中心治疗 HHT 患者的前瞻性数据表明,其死亡率与普通人群相似。然而,HHT 患者的临床表型差异很大,可能会影响死亡率。我们旨在测量中心治疗的 HHT 患者的死亡预测因素。自 2010 年以来,HHT 患者在脑血管畸形联盟(BVMC)的 14 个 HHT 中心被招募,并每年进行随访。在基线和随访期间收集生命状态、器官血管畸形(VM)和临床症状数据(N=1286)。我们使用 Cox 回归分析测试了器官 VM、HHT 症状和 HHT 基因是否与死亡率增加相关,同时调整了患者的年龄、性别和吸烟状况。
在平均 3.4 年(最长 8.6 年)的随访期间,有 59 人死亡。贫血史与死亡率增加相关(HR=2.93,95%CI 1.37-6.26,p=0.006),胃肠道(GI)出血(HR=2.63,95%CI 1.46-4.74,p=0.001)和有症状的肝 VM(HR=2.10,95%CI 1.15-3.84,p=0.015)也是如此。脑 VM 和肺动静脉畸形(AVM)与死亡率无关(p>0.05)。SMAD4 突变患者的死亡率明显更高(HR=18.36,95%CI 5.60-60.20,p<0.001),而 ACVRL1 或 ENG 突变患者则没有(n=33,4 例死亡)。
慢性胃肠道出血、贫血和有症状的肝 VM 与 HHT 患者的死亡率增加相关,与年龄无关,这与这些 HHT 方面的有限治疗选择一致。相反,肺 AVM 或脑 VM 似乎与死亡率无关,因为这些患者会在 HHT 中心进行常规筛查和预防性治疗。这表明需要开发新的治疗方法来治疗慢性贫血、胃肠道出血和有症状的肝 VM,以降低 HHT 患者的死亡率。