Department of Thoracic Medicine, Chang Gung Memorial Hospital, Chang Gung University College of Medicine, Linkou, No. 5, Fu-Shing St., GuiShan, Taoyuan, Taiwan.
Graduate Institute of Clinical Medical Sciences, College of Medicine, Chang Gung University, Taoyuan, Taiwan.
Crit Care. 2021 Jan 6;25(1):13. doi: 10.1186/s13054-020-03428-x.
Mechanical power (MP) refers to the energy delivered by a ventilator to the respiratory system per unit of time. MP referenced to predicted body weight (PBW) or respiratory system compliance have better predictive value for mortality than MP alone in acute respiratory distress syndrome (ARDS). Our objective was to assess the potential impact of consecutive changes of MP on hospital mortality among ARDS patients receiving extracorporeal membrane oxygenation (ECMO).
We performed a retrospective analysis of patients with severe ARDS receiving ECMO in a tertiary care referral center in Taiwan between May 2006 and October 2015. Serial changes of MP during ECMO were recorded.
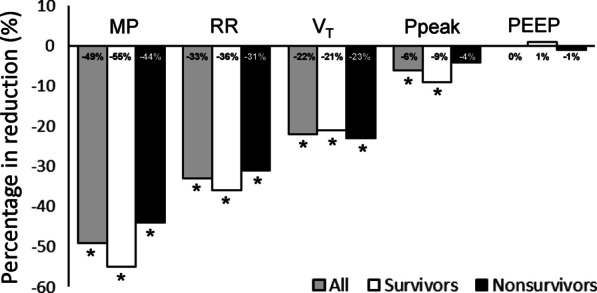
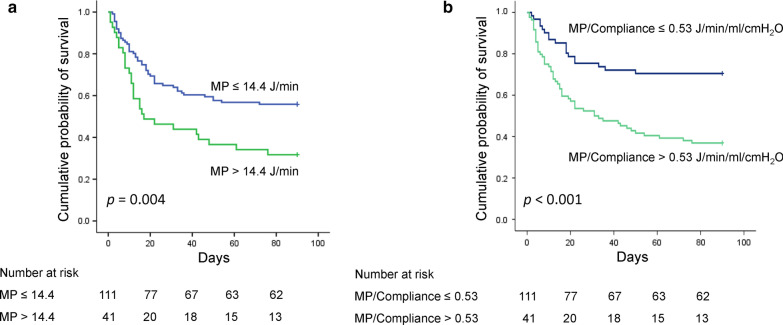
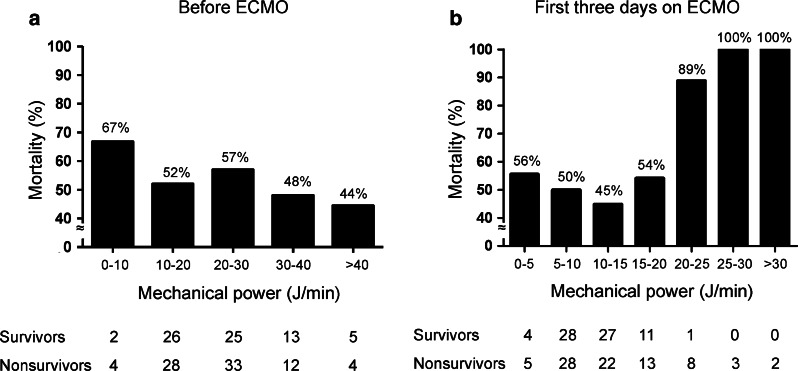
A total of 152 patients with severe ARDS rescued with ECMO were analyzed. Overall hospital mortality was 53.3%. There were no significant differences between survivors and nonsurvivors in terms of baseline values of MP or other ventilator settings. Cox regression models demonstrated that mean MP alone, MP referenced to PBW, and MP referenced to compliance during the first 3 days of ECMO were all independently associated with hospital mortality. Higher MP referenced to compliance (HR 2.289 [95% CI 1.214-4.314], p = 0.010) was associated with a higher risk of death than MP itself (HR 1.060 [95% CI 1.018-1.104], p = 0.005) or MP referenced to PBW (HR 1.004 [95% CI 1.002-1.007], p < 0.001). The 90-day hospital mortality of patients with high MP (> 14.4 J/min) during the first 3 days of ECMO was significantly higher than that of patients with low MP (≦ 14.4 J/min) (70.7% vs. 46.8%, p = 0.004), and the 90-day hospital mortality of patients with high MP referenced to compliance (> 0.53 J/min/ml/cm HO) during the first 3 days of ECMO was significantly higher than that of patients with low MP referenced to compliance (≦ 0.53 J/min/ml/cm HO) (63.6% vs. 29.7%, p < 0.001).
MP during the first 3 days of ECMO was the only ventilatory variable independently associated with 90-day hospital mortality, and MP referenced to compliance during ECMO was more predictive for mortality than was MP alone.
机械功率(MP)是指单位时间内呼吸机输送给呼吸系统的能量。在急性呼吸窘迫综合征(ARDS)中,MP 参考预测体重(PBW)或呼吸系统顺应性比单独的 MP 具有更好的死亡率预测价值。我们的目的是评估 ARDS 患者接受体外膜肺氧合(ECMO)治疗时,MP 连续变化对住院死亡率的潜在影响。
我们对 2006 年 5 月至 2015 年 10 月在台湾一家三级转诊中心接受 ECMO 治疗的严重 ARDS 患者进行了回顾性分析。记录 ECMO 期间 MP 的连续变化。
共分析了 152 例接受 ECMO 治疗的严重 ARDS 患者。总体住院死亡率为 53.3%。幸存者和非幸存者在 MP 或其他呼吸机设置的基线值方面没有显著差异。Cox 回归模型表明,ECMO 前 3 天的平均 MP、MP 参考 PBW 和 MP 参考顺应性均与住院死亡率独立相关。与 MP 本身(HR 1.060 [95% CI 1.018-1.104],p=0.005)或 MP 参考 PBW(HR 1.004 [95% CI 1.002-1.007],p<0.001)相比,MP 参考顺应性(HR 2.289 [95% CI 1.214-4.314],p=0.010)与死亡风险增加相关。ECMO 前 3 天 MP(>14.4 J/min)较高的患者 90 天住院死亡率明显高于 MP 较低的患者(≦14.4 J/min)(70.7% vs. 46.8%,p=0.004),而 MP 参考顺应性(>0.53 J/min/ml/cm HO)较高的患者 90 天住院死亡率明显高于 MP 参考顺应性较低的患者(≦0.53 J/min/ml/cm HO)(63.6% vs. 29.7%,p<0.001)。
ECMO 前 3 天的 MP 是唯一与 90 天住院死亡率独立相关的通气变量,MP 参考顺应性比单独的 MP 更能预测死亡率。