Silva Pedro Leme, Ball Lorenzo, Rocco Patricia R M, Pelosi Paolo
Laboratory of Pulmonary Investigation, Centro de Ciências da Saúde, Carlos Chagas Filho Institute of Biophysics, Federal University of Rio de Janeiro, Av. Carlos Chagas Filho, s/n, Bloco G-014, Ilha do Fundão, Rio de Janeiro, RJ, 21941-902, Brazil.
Department of Surgical Sciences and Integrated Diagnostics (DISC), University of Genoa, Largo Rosanna Benzi, 8, 16131, Genoa, Italy.
Intensive Care Med Exp. 2019 Jul 25;7(Suppl 1):38. doi: 10.1186/s40635-019-0243-4.
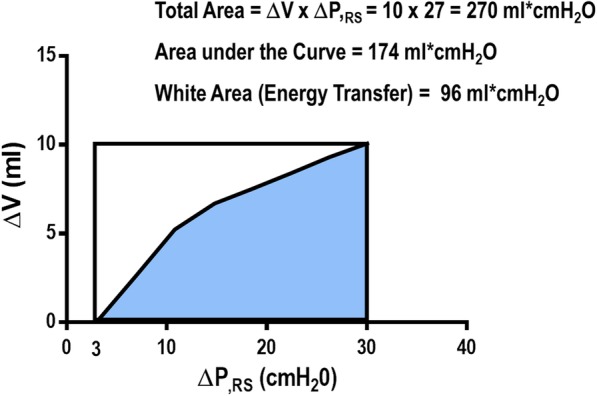
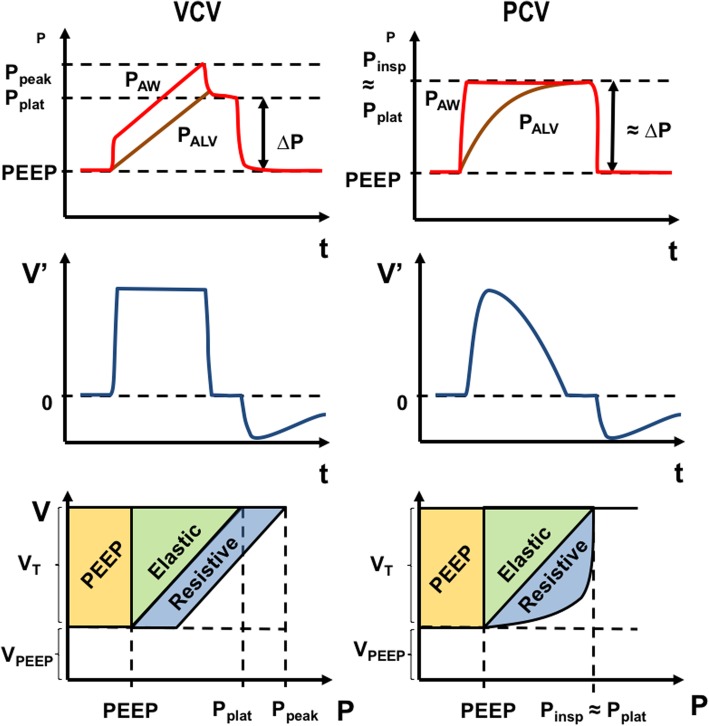
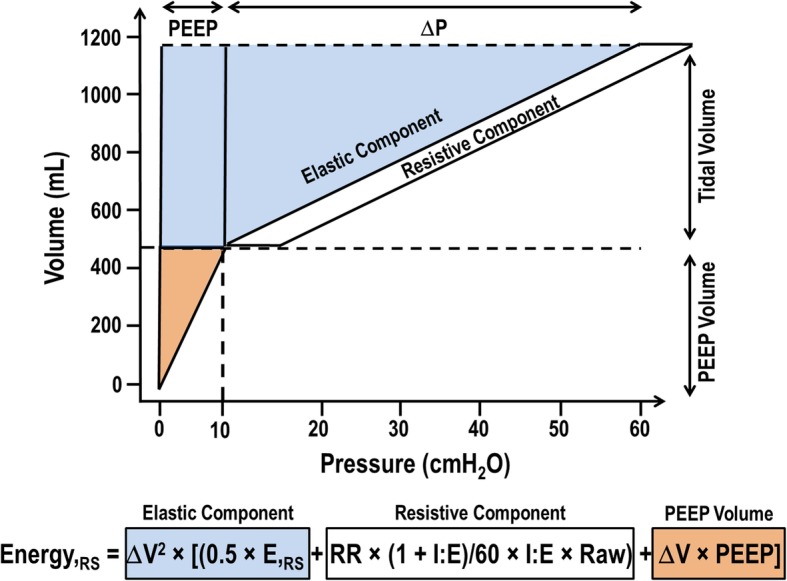
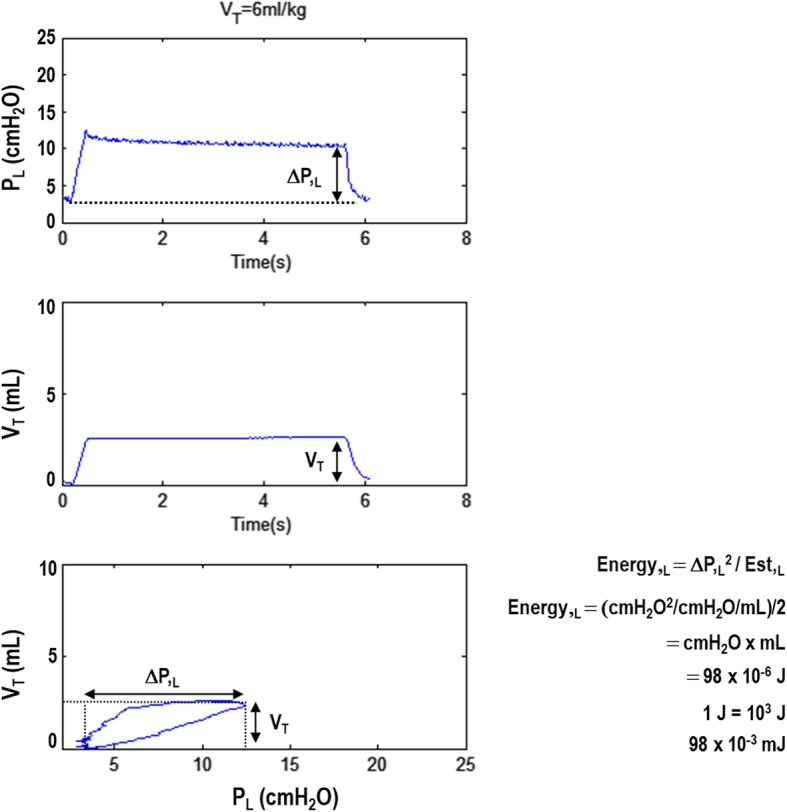
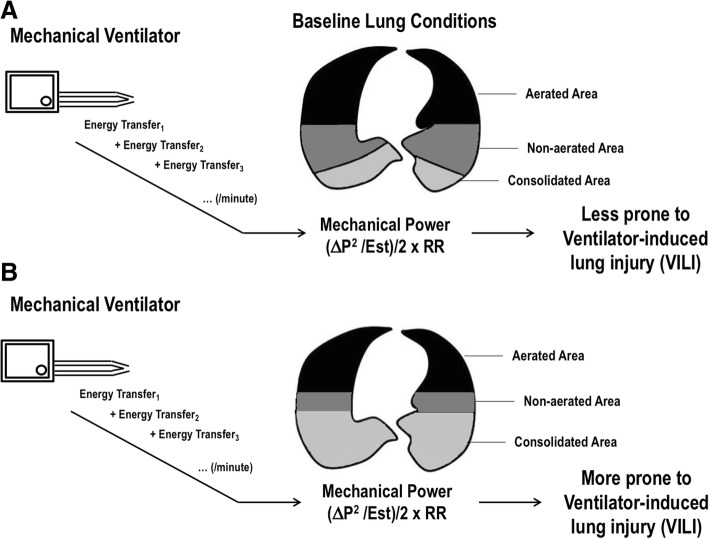
Mechanical ventilation is a life-supportive therapy, but can also promote damage to pulmonary structures, such as epithelial and endothelial cells and the extracellular matrix, in a process referred to as ventilator-induced lung injury (VILI). Recently, the degree of VILI has been related to the amount of energy transferred from the mechanical ventilator to the respiratory system within a given timeframe, the so-called mechanical power. During controlled mechanical ventilation, mechanical power is composed of parameters set by the clinician at the bedside-such as tidal volume (V), airway pressure (Paw), inspiratory airflow (V'), respiratory rate (RR), and positive end-expiratory pressure (PEEP) level-plus several patient-dependent variables, such as peak, plateau, and driving pressures. Different mathematical equations are available to calculate mechanical power, from pressure-volume (PV) curves to more complex formulas which consider both dynamic (kinetic) and static (potential) components; simpler methods mainly consider the dynamic component. Experimental studies have reported that, even at low levels of mechanical power, increasing V causes lung damage. Mechanical power should be normalized to the amount of ventilated pulmonary surface; the ratio of mechanical power to the alveolar area exposed to energy delivery is called "intensity." Recognizing that mechanical power may reflect a conjunction of parameters which may predispose to VILI is an important step toward optimizing mechanical ventilation in critically ill patients. However, further studies are needed to clarify how mechanical power should be taken into account when choosing ventilator settings.
机械通气是一种维持生命的治疗方法,但在一个被称为呼吸机诱导性肺损伤(VILI)的过程中,也会促进对肺部结构的损伤,如上皮细胞、内皮细胞和细胞外基质。最近,VILI的程度与在给定时间内从机械通气机传递到呼吸系统的能量数量有关,即所谓的机械功率。在控制机械通气期间,机械功率由临床医生在床边设置的参数组成,如潮气量(V)、气道压力(Paw)、吸气气流(V')、呼吸频率(RR)和呼气末正压(PEEP)水平,再加上几个与患者相关的变量,如峰值压力、平台压力和驱动压力。有不同的数学方程可用于计算机械功率,从压力-容积(PV)曲线到更复杂的公式,这些公式同时考虑了动态(动能)和静态(势能)成分;更简单的方法主要考虑动态成分。实验研究报告称,即使在低水平的机械功率下,增加V也会导致肺损伤。机械功率应根据通气的肺表面积进行归一化;机械功率与暴露于能量传递的肺泡面积之比称为“强度”。认识到机械功率可能反映了一系列可能导致VILI的参数的结合,这是朝着优化重症患者机械通气迈出的重要一步。然而,还需要进一步研究来阐明在选择通气机设置时应如何考虑机械功率。