Castro Madelyn, Venkateswaran Nisha, Peters Samuel T, Deyle David R, Bower Matthew, Koob Michael D, Boeve Bradley F, Vossel Keith
Department of Neurology, N. Bud Grossman Center for Memory Research and Care, University of Minnesota, Minneapolis, MN, United States.
Department of Neurology, Mary S. Easton Center for Alzheimer's Disease Research at UCLA, David Geffen School of Medicine at UCLA, Los Angeles, CA, United States.
Front Neurol. 2020 Dec 21;11:600468. doi: 10.3389/fneur.2020.600468. eCollection 2020.
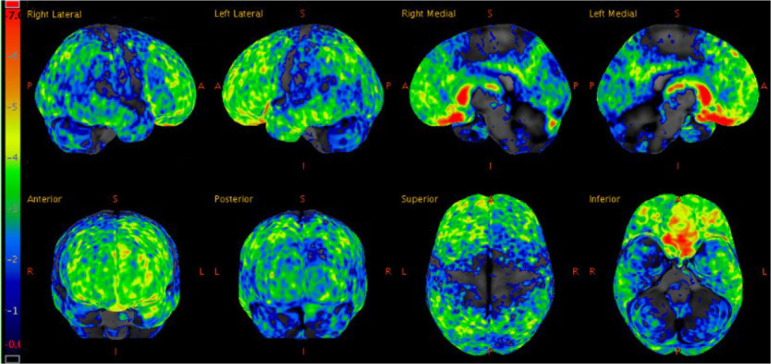
Frontotemporal dementia (FTD) rarely occurs in individuals under the age of 30, and genetic causes of early-onset FTD are largely unknown. The current report follows a 27 year-old patient with no significant past medical history presenting with two years of progressive changes in behavior, rushed speech, verbal aggression, and social withdrawal. MRI and FDG-PET imaging of the brain revealed changes maximally in the frontal and temporal lobes, which along with the clinical features, are consistent with behavioral variant FTD. Next generation sequencing of a panel of 28 genes associated with dementia and amyotrophic lateral sclerosis (ALS) initially revealed a duplication of exon 15 in (). Whole genome sequencing determined that this genetic anomaly was, in fact, a sequence corresponding with full-length variant 5 inserted into chromosome 12, indicating retrotransposition from a messenger RNA intermediate. To our knowledge, this is a novel mutation of , as the majority of mutations in linked to FTD-ALS are point mutations. Genomic DNA analysis revealed that this mutation is also present in one unaffected first-degree relative and one unaffected second-degree relative. This suggests that the mutation is either a disease-causing mutation with incomplete penetrance, which has been observed in heritable FTD, or a benign variant. Retrotransposons are not often implicated in neurodegenerative diseases; thus, it is crucial to clarify the potential role of this variant 5 retrotransposition in early-onset FTD.
额颞叶痴呆(FTD)在30岁以下的个体中很少发生,早发性FTD的遗传原因在很大程度上尚不清楚。本报告追踪了一名27岁的患者,该患者既往无重大病史,出现了两年的行为渐进性改变、语速加快、言语攻击性和社交退缩。脑部的MRI和FDG-PET成像显示额叶和颞叶变化最大,这与临床特征一起,符合行为变异型FTD。对一组与痴呆和肌萎缩侧索硬化症(ALS)相关的28个基因进行的下一代测序最初显示()外显子15重复。全基因组测序确定这种基因异常实际上是一个与插入12号染色体的全长变体5相对应的序列,表明是从信使RNA中间体反转录转座而来。据我们所知,这是一种新的(基因)突变,因为与FTD-ALS相关的(该基因)大多数突变是点突变。基因组DNA分析显示,这种突变也存在于一名未受影响的一级亲属和一名未受影响的二级亲属中。这表明该突变要么是一种具有不完全外显率的致病突变(遗传性FTD中已观察到),要么是一种良性变体。反转录转座子在神经退行性疾病中并不常见;因此,阐明这种变体5反转录转座在早发性FTD中的潜在作用至关重要。