Martinez-Perez Rafael, Tsimpas Asterios, Joswig Holger, Hernandez-Alvarez Victor, Mura Jorge
Department of Neurosurgery, University of Colorado, Aurora, Colorado, United States.
Department of Surgery, Advocate Illinois Masonic Center, Chicago, Illinois, United States.
Surg Neurol Int. 2020 Nov 11;11:382. doi: 10.25259/SNI_368_2020. eCollection 2020.
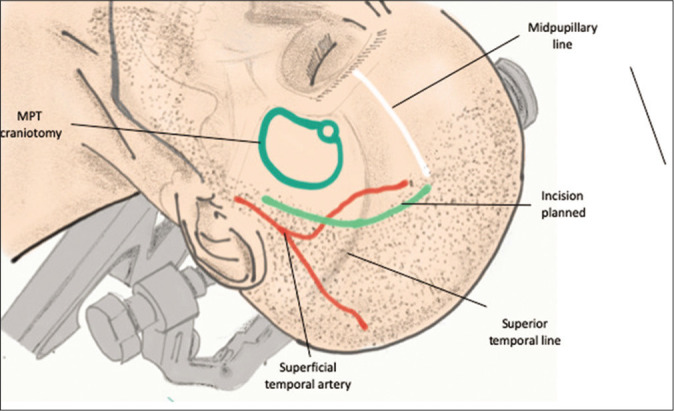
The clinical applicability of the minipterional (MPT) craniotomy is still limited to small and superficial anterior circulation aneurysms. We discuss the technical nuances of a modified MPT approach, the extradural MPT approach (eMPTa), for the treatment of a giant intracranial aneurysm (GIA) arising from the paraclinoid carotid artery.
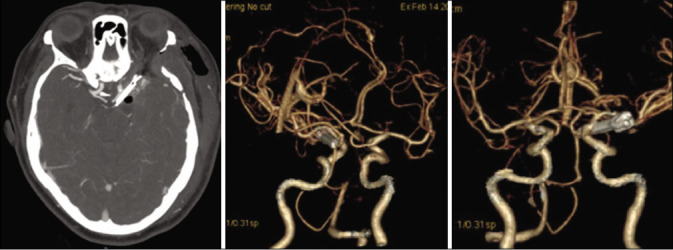
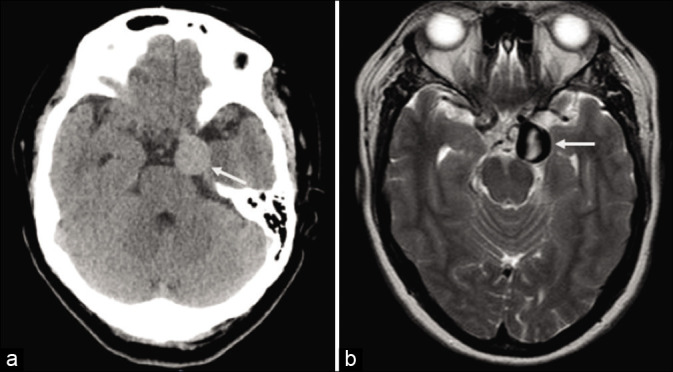
A 44-year-old female presented with facial hypoesthesia and third cranial nerve palsy. Further investigations revealed the presence of a 27 mm aneurysm arising from the communicating segment of the internal carotid artery. The patient underwent surgical clipping through an extradural MPT craniotomy and combined anterior clinoidectomy. Postoperative angio-computed tomography demonstrated complete aneurysm occlusion and patency of the parent vessels. The patient recovered fully from her previous deficits.
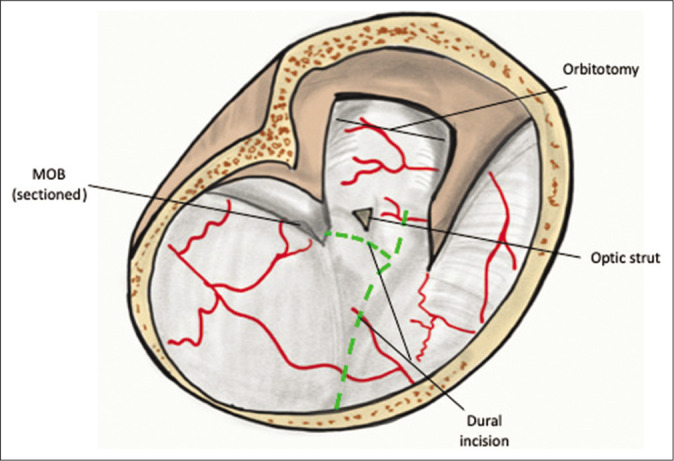
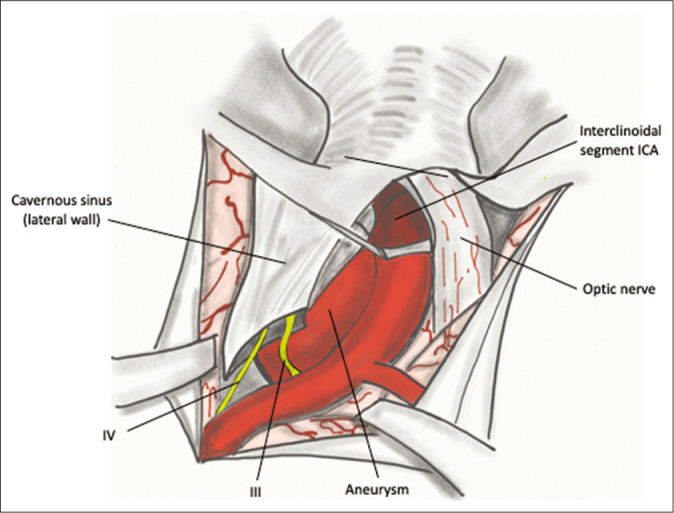
The skull base drilling, interdural dissection, and anterior clinoidectomy are key steps during the eMPTa that optimizes the use of the extradural corridor. Such adaptations are enough to improve the surgical maneuverability along the paraclinoid region and adapt the MPT suitability for the treatment of complex GIA.
翼点小骨窗开颅术(MPT)的临床适用性仍局限于小型及表浅的前循环动脉瘤。我们探讨一种改良的MPT入路,即硬膜外MPT入路(eMPTa),用于治疗起源于床突旁颈内动脉的巨大颅内动脉瘤(GIA)的技术细节。
一名44岁女性,出现面部感觉减退及动眼神经麻痹。进一步检查发现颈内动脉交通段有一个27毫米的动脉瘤。该患者接受了硬膜外MPT开颅及联合前床突切除术的手术夹闭。术后血管计算机断层扫描显示动脉瘤完全闭塞且载瘤血管通畅。患者先前的功能缺损完全恢复。
颅底钻孔、硬膜间分离及前床突切除术是eMPTa过程中的关键步骤,这些步骤优化了硬膜外通道的使用。这些改进足以提高沿床突旁区域的手术可操作性,并使MPT更适合治疗复杂的GIA。