Toma Miki, Yanai Toshihiro, Yoshida Shiho
Department of Pediatric Surgery, Ibaraki Children's Hospital, 3-3-1, Futabadai, Mito, Ibaraki, 311-4145, Japan.
Surg Case Rep. 2021 Jan 6;7(1):4. doi: 10.1186/s40792-020-01087-2.
The management of large abdominal wall defects, such as omphalocele or gastroschisis, remains a challenge for pediatric surgeons. Though several techniques have been described to repair those conditions, there is no procedure considered to be the standard worldwide. We report an infant girl with a giant ventral hernia after staged surgery for omphalocele in whom delayed closure of a large abdominal wall defect was performed successfully using "endoscopic component separation technique (ECST)" without serious complications.
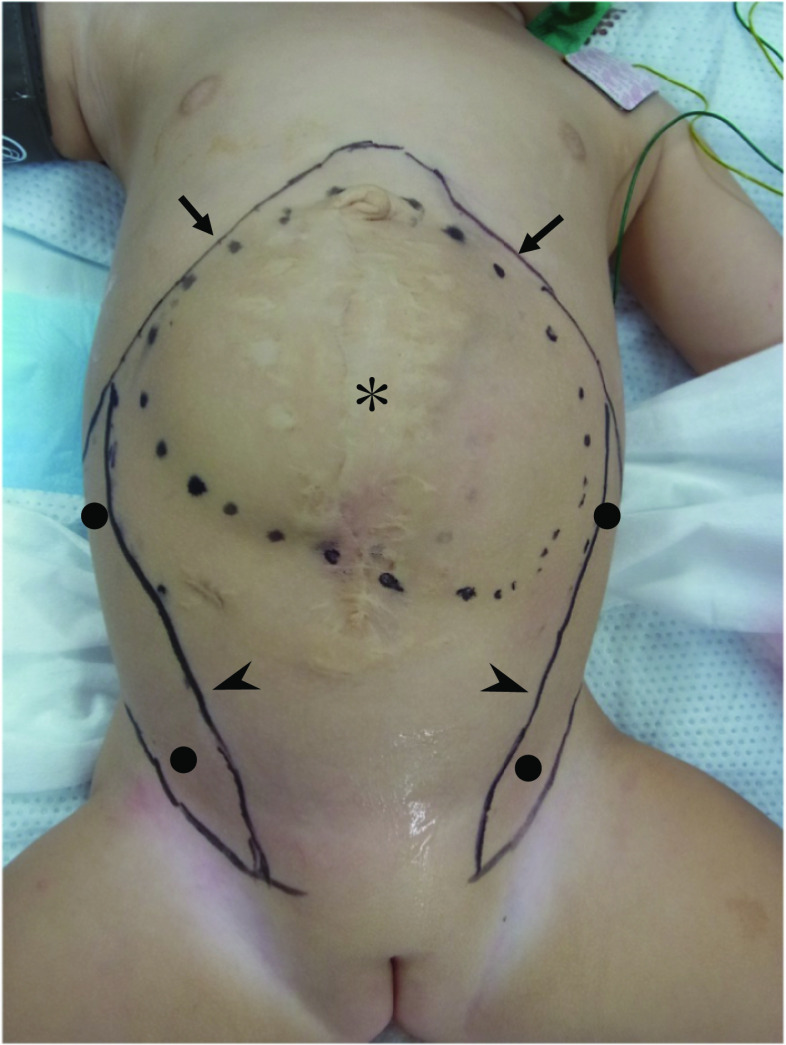
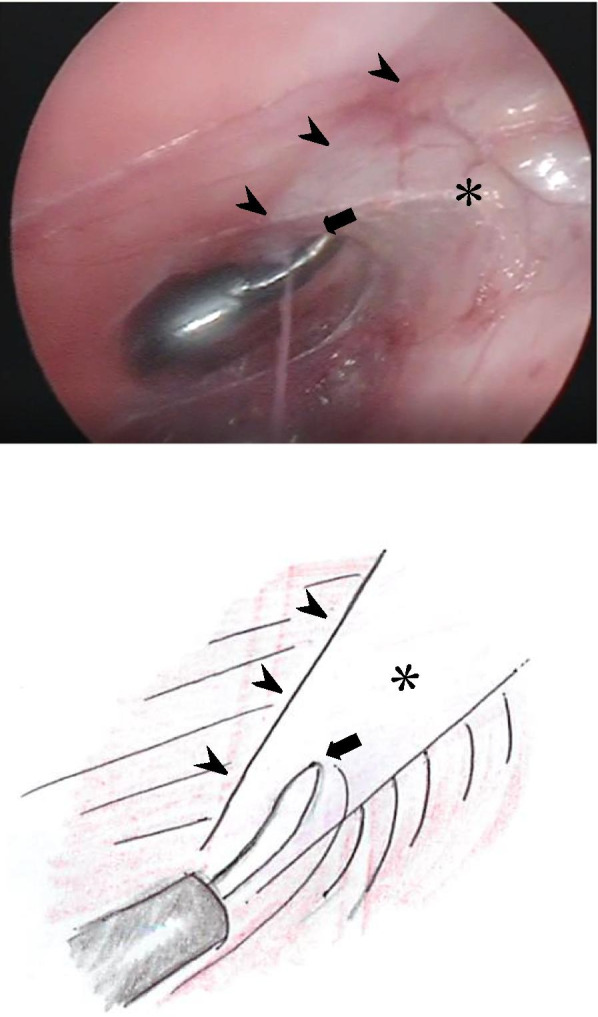
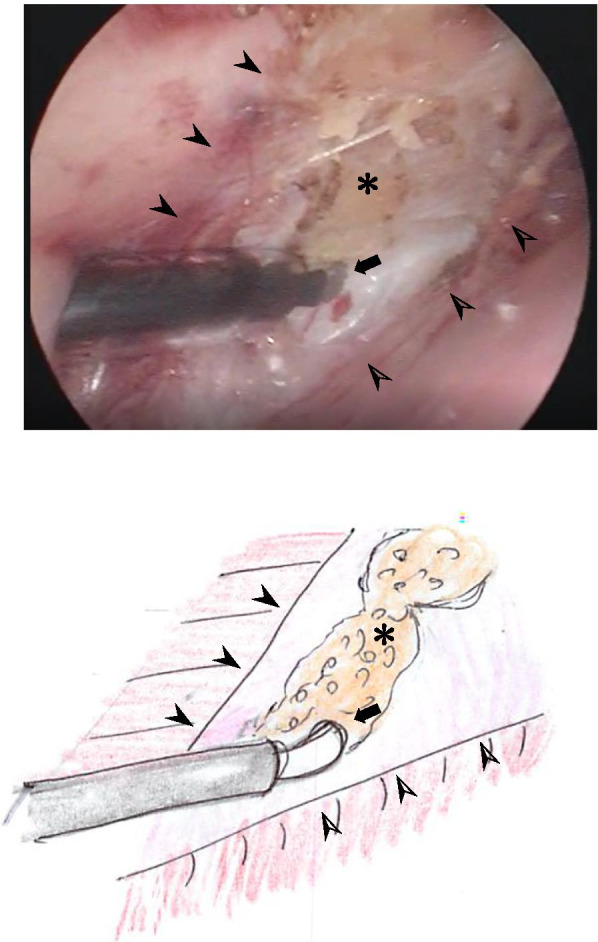
A baby girl was admitted to our hospital because of a giant omphalocele, which had been prenatally diagnosed. The omphalocele was supraumbilical and included the entire liver. After staged surgery, a large abdominal wall defect was closed by skin, creating a giant ventral hernia. We performed endoscopic separation component technique (ECST) for the closure of her abdominal wall defect when she was 11 months of age. ECST was initiated with placement of a 5.0-mm port just above the inguinal ligament and under the external oblique muscle. The space between the external and internal oblique muscles was created by the insufflation pressure, and a second 5.0-mm port was placed at 1.0 cm below the inferior edge of the rib into the space. As the further dissection was carried, the aponeurosis of the external oblique muscle was identified as a white line, running vertically from the epigastrium to inguinal ligament. It was transected longitudinally using electrocautery over its full length. The same procedure was performed on the contralateral side and the abdominal wall was successfully closed. Postoperative course was uneventful.
The technique of ECST, described here, is simple and safe for infants, and the cosmetic result is satisfactory.
大型腹壁缺损,如脐膨出或腹裂的处理,对小儿外科医生来说仍然是一项挑战。尽管已有多种技术用于修复这些病症,但尚无一种被认为是全球标准的手术方法。我们报告了一名婴儿女孩,她在接受脐膨出分期手术后出现巨大腹侧疝,采用“内镜下成分分离技术(ECST)”成功进行了大型腹壁缺损的延迟关闭,且未出现严重并发症。
一名因巨大脐膨出入院的女婴,该脐膨出在产前已被诊断。脐膨出位于脐上,包含整个肝脏。分期手术后,腹壁缺损用皮肤关闭,形成巨大腹侧疝。当她11个月大时,我们采用内镜分离成分技术(ECST)来关闭其腹壁缺损。ECST开始时,在腹股沟韧带上方、腹外斜肌下方置入一个5.0毫米的端口。通过气腹压力在腹外斜肌和腹内斜肌之间形成空间,并在肋骨下缘下方1.0厘米处向该空间置入第二个5.0毫米的端口。随着进一步的解剖,腹外斜肌腱膜被识别为一条从腹上区垂直延伸至腹股沟韧带的白线。使用电灼术在其全长范围内纵向切断。对侧进行相同操作,腹壁成功关闭。术后过程顺利。
本文所述的ECST技术对婴儿来说简单且安全,美容效果令人满意。