Dossa Fahima, Megetto Olivia, Yakubu Mafo, Zhang David D Q, Baxter Nancy N
Division of General Surgery, Department of Surgery, University of Toronto, Toronto, ON, Canada.
Institute of Health Policy, Management, and Evaluation, Dalla Lana School of Public Health, University of Toronto, Toronto, ON, Canada.
BMC Gastroenterol. 2021 Jan 7;21(1):22. doi: 10.1186/s12876-020-01561-z.
Sedation is commonly used in gastrointestinal endoscopy; however, considerable variability in sedation practices has been reported. The objective of this review was to identify and synthesize existing recommendations on sedation practices for routine gastrointestinal endoscopy procedures.
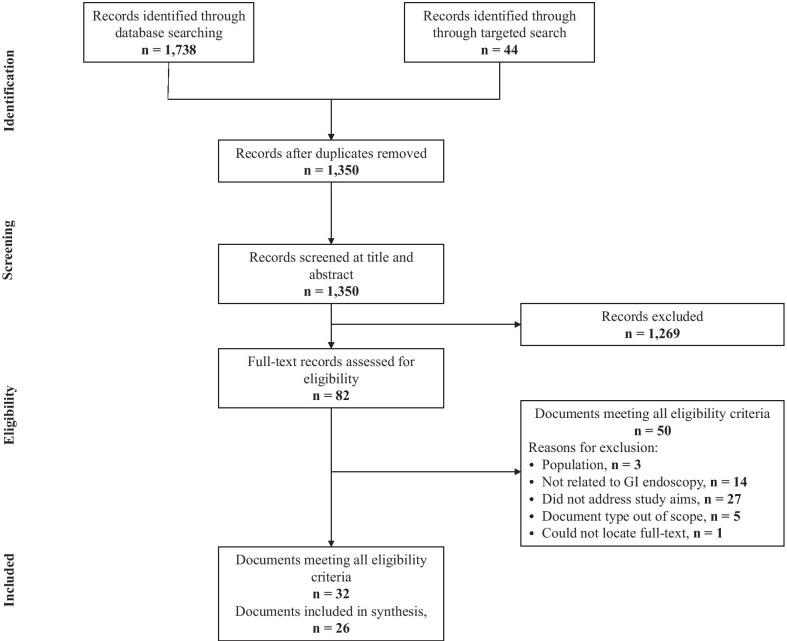
We systematically reviewed guidelines and position statements identified through a search of PubMed, guidelines databases, and websites of relevant professional associations from January 1, 2005 to May 10, 2019. We included English-language guidelines/position statements with recommendations relating to sedation for adults undergoing routine gastrointestinal endoscopy. Documents with guidance only for complex endoscopic procedures were excluded. We extracted and synthesized recommendations relating to: 1) choice of sedatives, 2) sedation administration, 3) personnel responsible for monitoring sedated patients, 4) skills and training of individuals involved in sedation, and 5) equipment required for monitoring sedated patients. We assessed the quality of included documents using the Appraisal of Guidelines for Research & Evaluation (AGREE) II tool.
We identified 19 guidelines and 7 position statements meeting inclusion criteria. Documents generally agreed that a single, trained registered nurse can administer moderate sedation, monitor the patient, and assist with brief, interruptible tasks. Documents also agreed on the routine use of pulse oximetry and blood pressure monitoring during endoscopy. However, recommendations relating to the drugs to be used for sedation, the healthcare personnel capable of administering propofol and monitoring patients sedated with propofol, and the need for capnography when monitoring sedated patients varied. Only 9 documents provided a grade or level of evidence in support of their recommendations.
Recommendations for sedation practices in routine gastrointestinal endoscopy differ across guidelines/position statements and often lack supporting evidence with potential implications for patient safety and procedural efficiency.
镇静常用于胃肠内镜检查;然而,已有报道称镇静操作存在相当大的变异性。本综述的目的是识别并综合关于常规胃肠内镜检查镇静操作的现有建议。
我们系统回顾了2005年1月1日至2019年5月10日期间通过检索PubMed、指南数据库以及相关专业协会网站所确定的指南和立场声明。我们纳入了与接受常规胃肠内镜检查的成人镇静相关建议的英文指南/立场声明。仅针对复杂内镜手术的指导性文件被排除。我们提取并综合了与以下方面相关的建议:1)镇静剂的选择,2)镇静给药,3)负责监测镇静患者的人员,4)参与镇静的人员的技能和培训,以及5)监测镇静患者所需的设备。我们使用研究与评估指南评估(AGREE)II工具评估纳入文件的质量。
我们确定了19项指南和7项立场声明符合纳入标准。文件普遍认为,一名经过培训的注册护士可以实施中度镇静、监测患者并协助完成简短的、可中断的任务。文件还一致同意在内镜检查期间常规使用脉搏血氧饱和度测定和血压监测。然而,关于用于镇静的药物、能够使用丙泊酚并监测丙泊酚镇静患者的医护人员以及监测镇静患者时是否需要二氧化碳监测的建议各不相同。只有9份文件提供了支持其建议的证据等级或水平。
常规胃肠内镜检查镇静操作的建议在不同的指南/立场声明中存在差异,且往往缺乏支持证据,这可能对患者安全和操作效率产生影响。