Karakawa Ryo, Yoshimatsu Hidehiko, Maeda Erisa, Shibata Tomoyoshi, Tanakura Kenta, Kuramoto Yukiko, Miyashita Hiroki, Yano Tomoyuki
Department of Plastic and Reconstructive Surgery, Cancer Institute Hospital of the Japanese Foundation for Cancer Research, Koto-ku, Tokyo, Japan.
Plast Reconstr Surg Glob Open. 2020 Dec 17;8(12):e3289. doi: 10.1097/GOX.0000000000003289. eCollection 2020 Dec.
Soft tissue sarcomas are rare neoplasms that can occur on any part of the body. The operative position for the resection is determined depending on the site of the soft tissue sarcomas; intraoperative repositioning may be needed for reconstruction. We present the profunda femoris artery perforator (PAP) flap harvest technique (wherein the flap can be used in any position), and suggest that the PAP flap transfer can eliminate the need for intraoperative repositioning.
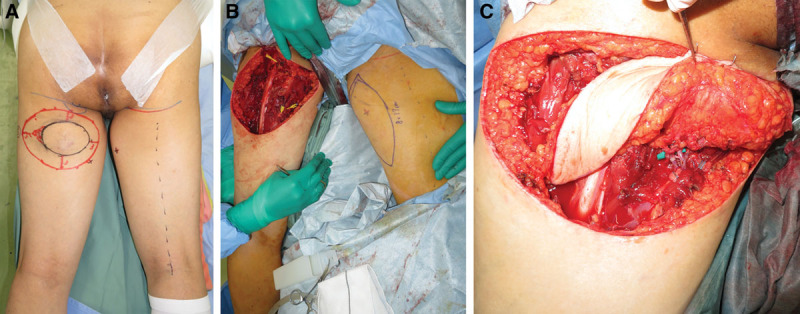
From December 2018 to January 2020, 7 patients with an average age of 68 years underwent reconstructions using a PAP flap after wide resection of STS. The mean defect size was 11.3 × 16.5 cm (range, 5.5-25 × 11-26 cm). The location of the defects was the medial thigh in 2 patients, the posterior thigh in 1, the popliteal fossa in 1, the groin in 1, and the buttock in 2. The PAP flap was elevated in the supine "frog-leg" position, the prone position, the jack-knife position, or the lateral "crisscross" position; the lateral decubitus position with the donor lower extremity on the bottom.
Of the 7 cases, the operations were performed in the supine "frog-leg" position in 3 cases, the prone position in 2 cases, the jack-knife position in 1 case, and the lateral "crisscross" position in 1 case. There were no intraoperative position changes in all cases. The mean size of the PAP flap was 8.7 × 19.9 cm (range, 6-11 × 17-24 cm). One patient had donor site dehiscence, which was treated conservatively. The PAP flaps survived completely in all cases. The mean follow-up period was 10.5 months (range, 6-17 months).
Since the PAP flap elevation is feasible in every position, the PAP flap can be considered a versatile reconstruction option after sarcoma resection.
软组织肉瘤是一种罕见的肿瘤,可发生于身体的任何部位。软组织肉瘤切除的手术体位取决于其所在部位;重建时可能需要术中重新定位。我们介绍了股深动脉穿支(PAP)皮瓣切取技术(该皮瓣可用于任何体位),并认为PAP皮瓣转移可避免术中重新定位的需要。
2018年12月至2020年1月,7例平均年龄68岁的患者在广泛切除软组织肉瘤后使用PAP皮瓣进行重建。平均缺损大小为11.3×16.5cm(范围5.5 - 25×11 - 26cm)。缺损部位为大腿内侧2例、大腿后侧1例、腘窝1例、腹股沟1例、臀部2例。PAP皮瓣在仰卧“蛙腿”位、俯卧位、折刀位或侧“交叉”位掀起;供体下肢在下的侧卧位。
7例中,3例在仰卧“蛙腿”位进行手术,2例在俯卧位,1例在折刀位,1例在侧“交叉”位。所有病例术中均未改变体位。PAP皮瓣平均大小为8.7×19.9cm(范围6 - 11×17 - 24cm)。1例患者供区裂开,保守治疗。所有病例中PAP皮瓣均完全存活。平均随访期为10.5个月(范围6 - 17个月)。
由于PAP皮瓣在每个体位均可掀起,PAP皮瓣可被视为肉瘤切除术后一种通用的重建选择。