Department of Pediatrics, Emory University School of Medicine, Atlanta, GA, USA.
Center for Childhood Infections and Vaccines of Children's Healthcare of Atlanta and Emory University, Atlanta, GA, USA.
Curr HIV/AIDS Rep. 2021 Apr;18(2):117-127. doi: 10.1007/s11904-020-00540-z. Epub 2021 Jan 12.
For most people living with HIV (PLWH), treatment with effective antiretroviral therapy (ART) results in suppression of viremia below the limit of detection of clinical assays, immune reconstitution, reduced immune activation, avoidance of opportunistic infections, and progression to AIDS. However, ART alone is not curative, and HIV persists in a non-replicating, latent form. In this review, we provide a historical perspective on non-specific latency reversal approaches (LRA 1.0) and summarize recent advances in latency reversal strategies that target specific signaling pathways within CD4+ T cells or other immune cells to induce expression of latent HIV (immune-based latency reversal, or LRA 2.0).
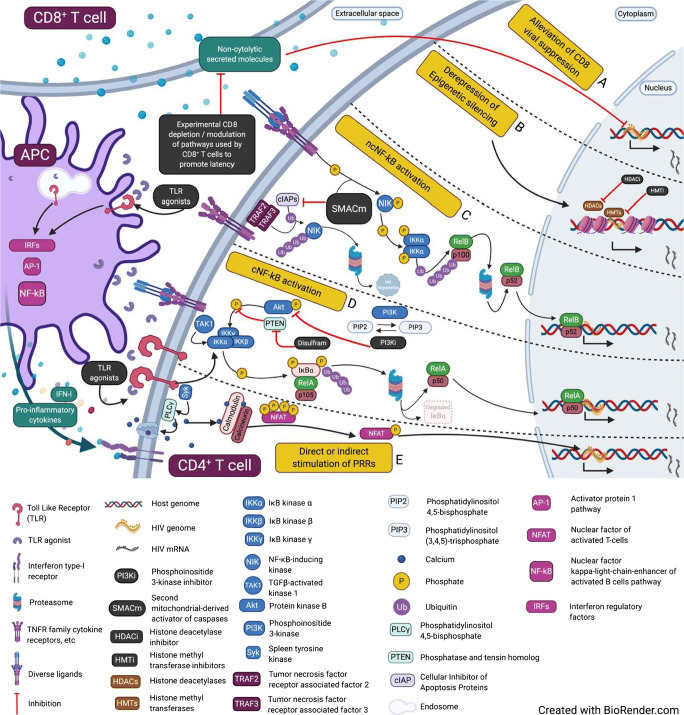
The HIV reservoir is primarily composed of latently infected CD4+ T cells carrying integrated, replication-competent provirus that can give rise to rebound viremia if ART is stopped. Myeloid lineage cells also contribute to HIV latency in certain tissues; we focus here on CD4+ T cells as a sufficient body of evidence regarding latency reversal in myeloid cells is lacking. The immunomodulatory LRA 2.0 approaches we describe include pattern recognition receptor agonists, immune checkpoint inhibitors, non-canonical NF-kB stimulation, and transient CD8+ lymphocyte depletion, along with promising combination strategies. We highlight recent studies demonstrating robust latency reversal in nonhuman primate models. While significant strides have been made in terms of virus reactivation from latency, initial hopes for latency reversal alone to result in a reduction of infected cells, through viral cytopathic effect or an unboosted immune system, have not been realized and it seems clear that even effective latency reversal strategies will need to be paired with an approach that facilitates immune recognition and clearance of cells containing reactivated virus.
对于大多数 HIV 感染者(PLWH),有效的抗逆转录病毒治疗(ART)可使病毒血症受到抑制,低于临床检测下限,免疫重建,减少免疫激活,避免机会性感染,并进展为艾滋病。然而,单独的 ART 并不能治愈 HIV,HIV 以非复制、潜伏的形式存在。在这篇综述中,我们提供了非特异性潜伏逆转方法(LRA 1.0)的历史观点,并总结了最近靶向 CD4+T 细胞或其他免疫细胞内特定信号通路的潜伏逆转策略的进展,以诱导潜伏 HIV 的表达(免疫为基础的潜伏逆转,或 LRA 2.0)。
HIV 储存库主要由潜伏感染的 CD4+T 细胞组成,这些细胞携带整合的、有复制能力的前病毒,如果停止 ART,就会导致病毒血症反弹。髓系细胞也会导致某些组织中的 HIV 潜伏;我们在这里重点关注 CD4+T 细胞,因为缺乏关于髓系细胞潜伏逆转的充分证据。我们描述的免疫调节 LRA 2.0 方法包括模式识别受体激动剂、免疫检查点抑制剂、非经典 NF-kB 刺激和短暂的 CD8+淋巴细胞耗竭,以及有前途的组合策略。我们强调了最近的研究,这些研究证明了在非人类灵长类动物模型中潜伏逆转的强大作用。尽管在从潜伏中激活病毒方面取得了重大进展,但最初希望通过潜伏逆转单独减少受感染细胞,通过病毒细胞病变效应或未增强的免疫系统,并没有实现,而且似乎很清楚,即使是有效的潜伏逆转策略也需要与一种能够促进免疫识别和清除含有再激活病毒的细胞的方法相匹配。