Centre for Academic Primary Care, Bristol Medical School, University of Bristol, Canynge Hall, 39 Whatley Road, Bristol, BS8 2PS, UK.
School for Policy Studies, University of Bristol, Bristol, UK.
BMC Fam Pract. 2021 Jan 12;22(1):19. doi: 10.1186/s12875-020-01297-5.
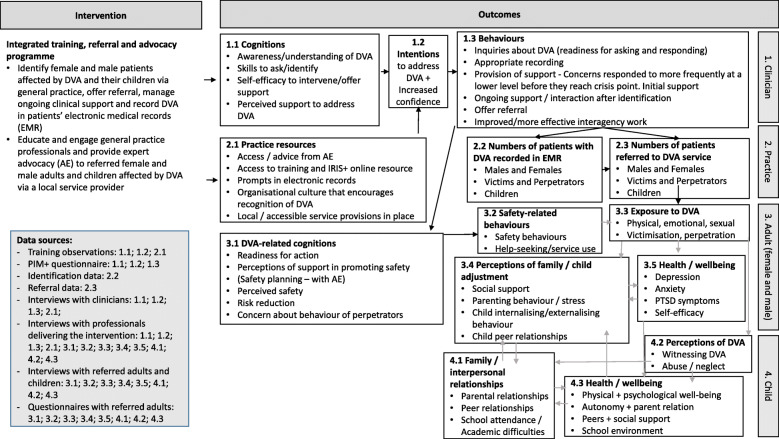
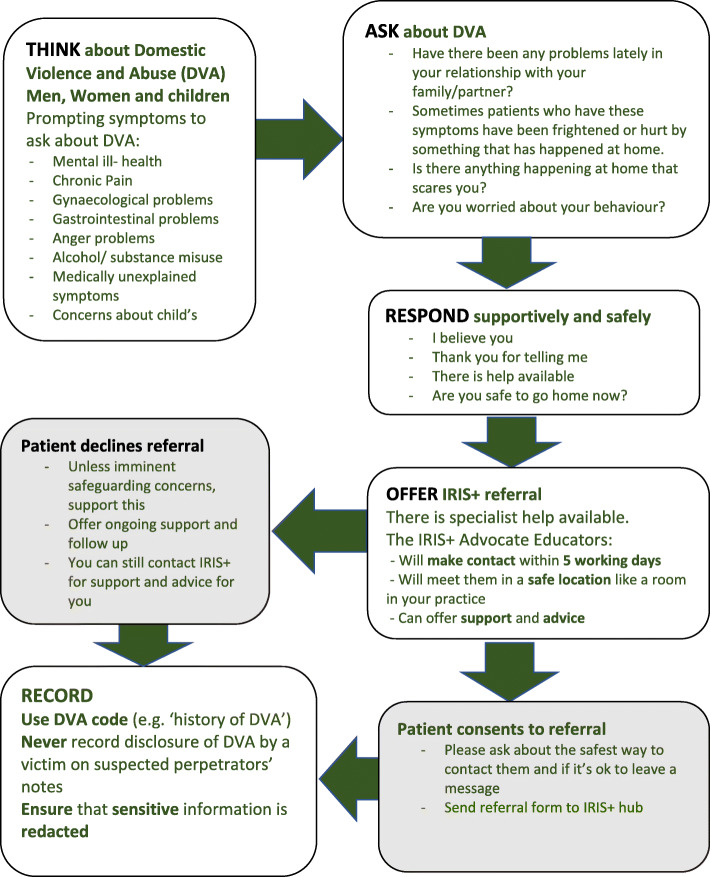
Primary care needs to respond effectively to patients experiencing or perpetrating domestic violence and abuse (DVA) and their children, but there is uncertainty about the value of integrated programmes. The aim of the study was to develop and test the feasibility of an integrated primary care system-level training and support intervention, called IRIS+ (Enhanced Identification and Referral to Improve Safety), for all patients affected by DVA. IRIS+ was an adaptation of the original IRIS (Identification and Referral to Improve Safety) model designed to reach female survivors of DVA.
Observation of training; pre/post intervention questionnaires with clinicians and patients; data extracted from medical records and DVA agency; semi-structured interviews with clinicians, service providers and referred adults and children. Data collection took place between May 2017 and April 2018. Mixed method analysis was undertaken to triangulate data from various sources to assess the feasibility and acceptability of the intervention.
Clinicians and service providers believed that the IRIS+ intervention had filled a service gap and was a valuable resource in identifying and referring women, men and children affected by DVA. Despite increased levels of preparedness reported by clinicians after training in managing the complexity of DVA in their practice, the intervention proved to be insufficient to catalyse identification and specialist referral of men and direct identification and referral (without their non-abusive parents) of children and young people. The study also revealed that reports provided to general practice by other agencies are important sources of information about adult and children patients affected by DVA. However, in the absence of guidance about how to use this information in patient care, there are uncertainties and variation in practice.
The study demonstrates that the IRIS+ intervention is not feasible in the form and timeframe we evaluated. Further adaptation is required to achieve identification and referral of men and children in primary care: an enhanced focus on engagement with men, direct engagement with children, and improved guidance and training on responding to reports of DVA received from other agencies.
初级保健需要有效应对经历或实施家庭暴力和虐待(DVA)的患者及其子女,但对于综合项目的价值存在不确定性。本研究旨在开发和测试一种名为 IRIS+(增强识别和转介以提高安全性)的综合初级保健系统层面培训和支持干预措施的可行性,该措施适用于所有受 DVA 影响的患者。IRIS+ 是最初的 IRIS(识别和转介以提高安全性)模型的改编版,旨在帮助 DVA 的女性幸存者。
观察培训;对临床医生和患者进行干预前后的问卷调查;从医疗记录和 DVA 机构中提取数据;对临床医生、服务提供者和转介的成年人和儿童进行半结构化访谈。数据收集于 2017 年 5 月至 2018 年 4 月之间进行。采用混合方法分析来对来自各种来源的数据进行三角分析,以评估干预措施的可行性和可接受性。
临床医生和服务提供者认为,IRIS+干预措施填补了服务空白,是识别和转介受 DVA 影响的妇女、男子和儿童的宝贵资源。尽管在培训后,临床医生报告在管理实践中的 DVA 复杂性方面的准备水平有所提高,但该干预措施证明不足以促进男性的识别和专家转介,以及儿童和青少年的直接识别和转介(无需其无虐待的父母)。研究还表明,其他机构向全科医生提供的报告是了解受 DVA 影响的成年和儿童患者的重要信息来源。然而,由于缺乏关于如何在患者护理中使用这些信息的指导,因此实践中存在不确定性和差异。
研究表明,我们评估的 IRIS+干预形式和时间框架不可行。需要进一步调整,以便在初级保健中实现对男性和儿童的识别和转介:更加强调与男性的接触、直接与儿童接触,以及改善对其他机构报告的 DVA 的反应的指导和培训。