Division of Infectious Diseases, Children's Hospital of Michigan, 3901 Beaubien Blvd, Detroit, MI, 48201, USA.
Wayne State University, Detroit, MI, USA.
Eur J Pediatr. 2021 May;180(5):1581-1591. doi: 10.1007/s00431-021-03935-1. Epub 2021 Jan 16.
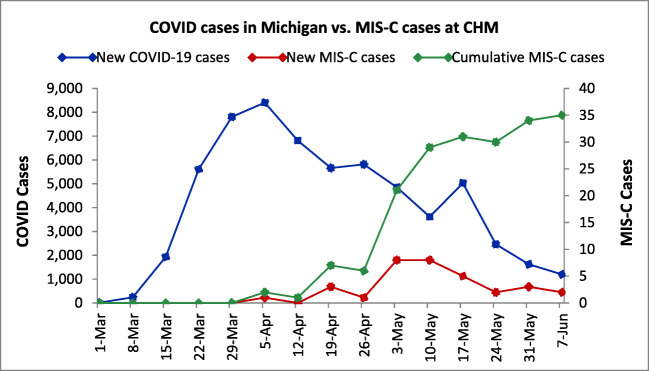
This study was conducted to assess the clinical spectrum, management, and outcome of SARS-CoV-2-related multisystem inflammatory syndrome in children (MIS-C). We reviewed medical records of children with MIS-C diagnosis seen at the Children's Hospital of Michigan in Detroit between April and June 2020. Thirty-three children were identified including 22 who required critical care (group 1) and 11 with less intense inflammation (group 2). Children in group 1 were older (median 7.0 years) than those in group 2 (median 2.0 years). Abdominal pain was present in 68% of patients in group 1. Hypotension or shock was present in 17/22 patients in group 1. Thirteen (39.4%) had Kawasaki disease (KD)-like manifestations. Five developed coronary artery dilatation; All resolved on follow-up. Intravenous immunoglobulin (IVIG) was given to all patients in group 1 and 7/11 in group 2. Second-line therapy was needed in 13/22 (group 1) for persisting inflammation or myocardial dysfunction; 12 received infliximab. All patients recovered.Conclusion: MIS-C clinical manifestations may overlap with KD; however, MIS-C is likely a distinct inflammatory process characterized by reversible myocardial dysfunction and rarely coronary artery dilatation. Supportive care, IVIG, and second-line therapy with infliximab were associated with a favorable outcome. What is Known: • Multisystem inflammatory syndrome in children (MIS-C) manifestations include fever, gastrointestinal symptoms, shock, and occasional features of Kawasaki disease (KD). • Treatment includes immunomodulatory agents, most commonly IVIG and corticosteroids. What is New: • Spectrum of MIS-C varies from mild to severe inflammation and coronary artery dilatation occurred in 5/22 (23%) critically ill patients. • IVIG and infliximab therapy were associated with a favorable outcome including resolution of coronary dilatation; only 2/33 received corticosteroids.
这项研究旨在评估儿童严重急性呼吸综合征冠状病毒 2 相关多系统炎症综合征(MIS-C)的临床特征、治疗方法和结局。我们回顾了 2020 年 4 月至 6 月期间在密歇根州底特律儿童医院就诊的 MIS-C 患儿的病历。共确定了 33 名患儿,其中 22 名患儿需要重症监护(第 1 组),11 名患儿炎症程度较轻(第 2 组)。第 1 组患儿年龄较大(中位数 7.0 岁),第 2 组患儿年龄较小(中位数 2.0 岁)。第 1 组患儿中有 68%存在腹痛症状。第 1 组 22 名患儿中有 17 名存在低血压或休克。13 名(39.4%)患儿有川崎病(KD)样表现。5 名患儿出现冠状动脉扩张;所有患儿在随访时均得到缓解。第 1 组患儿均接受静脉注射免疫球蛋白(IVIG)治疗,第 2 组患儿中有 7 名接受 IVIG 治疗。第 1 组中有 13 名(39.4%)患儿因炎症持续或心肌功能障碍需要二线治疗;其中 12 名患儿接受英夫利昔单抗治疗。所有患儿均康复。结论:MIS-C 的临床表现可能与 KD 重叠;然而,MIS-C 可能是一种以可逆性心肌功能障碍和罕见冠状动脉扩张为特征的独特炎症过程。支持治疗、IVIG 和英夫利昔单抗二线治疗与良好结局相关。已知:• 儿童多系统炎症综合征(MIS-C)的表现包括发热、胃肠道症状、休克和偶尔出现川崎病(KD)的特征。• 治疗包括免疫调节剂,最常用的是 IVIG 和皮质类固醇。新发现:• MIS-C 的表现范围从轻度到重度炎症,22 名重症患儿中有 5 名(23%)发生冠状动脉扩张。• IVIG 和英夫利昔单抗治疗与良好结局相关,包括冠状动脉扩张的缓解;仅 2/33 名患儿接受皮质类固醇治疗。