Smolic Milena, Sombroek Chèrita, Bloemers Monique C W M, van Triest Baukelien, Nowee Marlies E, Mans Anton
Department of Radiation Oncology, The Netherlands Cancer Institute, Amsterdam, the Netherlands.
Phys Imaging Radiat Oncol. 2019 Apr 24;10:14-18. doi: 10.1016/j.phro.2019.04.006. eCollection 2019 Apr.
Applying needles in the first brachytherapy (BT) fraction for patients with locally advanced cervical cancer allows for more dose conformality and OAR sparing, but is more challenging than in subsequent fractions, as pre-implant imaging with applicator is lacking. We investigate whether a needle simulation, a fixed needle configuration or a multidisciplinary discussion-based configuration can predict more accurately which applicator needle positions are best suited for use in the first BT fraction.
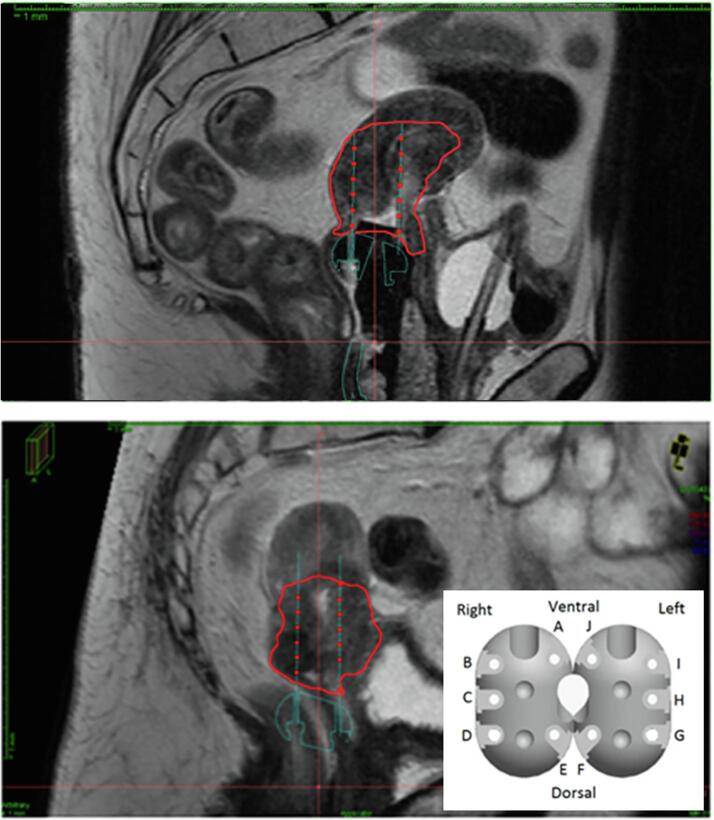
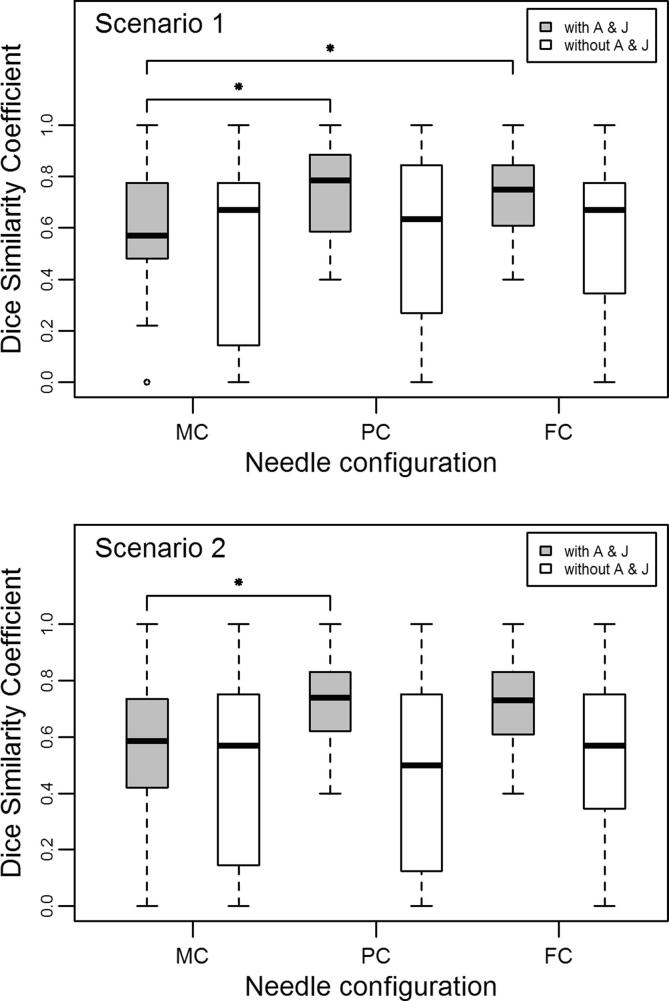
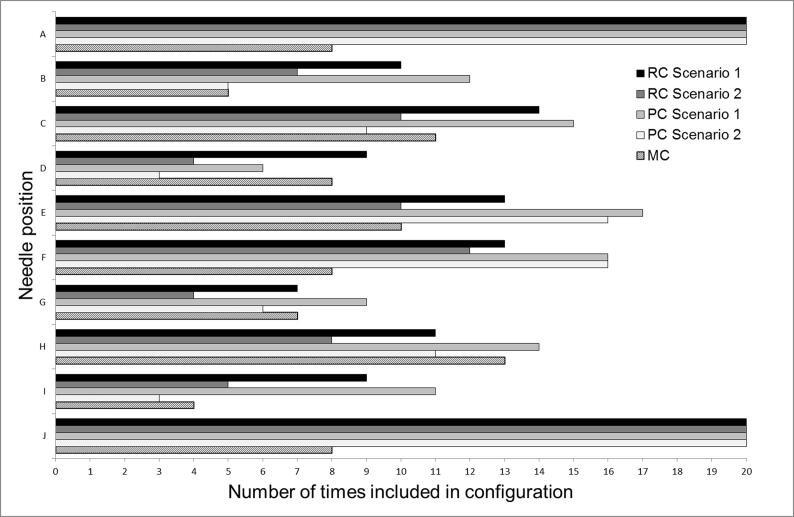
For 20 patients we retrospectively determined the "reference" needle configuration (RC) for the first BT fraction using magnetic resonance imaging (MRI) scans with applicator . We simulated a pre-MRI needle configuration (PC) using the MRI made in the fourth week of external beam radiotherapy (EBRT) without applicator . We generated a fixed needle configuration (FC) from the most common RC needles. Using Dice's similarity coefficient (DSC) we compared each of these needle configurations, including the clinically applied "multidisciplinary consensus" needle configuration (MC), with RC. We considered two scenarios: allowing up to ten needles (scenario 1), and limiting the needle number (scenario 2). The analysis was repeated omitting two mid-ventral needles previously determined as non-essential to treatment planning.
For both scenarios, the median DSC for PC and FC was higher than for MC (scenario1:DSC = 0,78; DSC = 0,75; DSC = 0,57; scenario 2:DSC = 0,74; DSC = 0,73; DSC = 0,59), while omitting mid-ventral needles resulted in no statistically significant differences in DSC.
The PC or FC method are at least as accurate as the MC, with the FC preferred for efficiency.
对于局部晚期宫颈癌患者,在首次近距离放疗(BT)时植入施源器可实现更好的剂量适形性并减少危及器官受量,但由于缺乏植入前施源器影像,这比后续分次放疗更具挑战性。我们研究了针模拟、固定针配置或基于多学科讨论的配置能否更准确地预测哪些施源器针位最适合首次BT分次放疗。
对于20例患者,我们使用带有施源器的磁共振成像(MRI)扫描回顾性确定首次BT分次放疗的“参考”针配置(RC)。我们在不使用施源器的情况下,利用外照射放疗(EBRT)第四周进行的MRI模拟植入前针配置(PC)。我们从最常见的RC针生成固定针配置(FC)。使用戴斯相似系数(DSC),我们将这些针配置中的每一种,包括临床应用的“多学科共识”针配置(MC),与RC进行比较。我们考虑了两种情况:允许最多十根针(情况1),以及限制针数(情况2)。分析重复进行,省略了先前确定对治疗计划非必需的两根腹侧中部针。
在两种情况下,PC和FC的DSC中位数均高于MC(情况1:DSC = 0.78;DSC = 0.75;DSC = 0.57;情况2:DSC = 0.74;DSC = 0.73;DSC = 0.59),而省略腹侧中部针导致DSC无统计学显著差异。
PC或FC方法至少与MC一样准确,FC因效率高而更受青睐。