Pedersen Jesper, Casares-Magaz Oscar, Petersen Jørgen B B, Rørvik Jarle, Bentzen Lise, Andersen Andreas G, Muren Ludvig P
Department of Medical Physics, Aarhus University Hospital/Aarhus University, Aarhus, Denmark.
Department of Clinical Medicine, University of Bergen and Department of Radiology, Haukeland University Hospital, Bergen, Norway.
Phys Imaging Radiat Oncol. 2018 Jul 18;6:101-105. doi: 10.1016/j.phro.2018.06.002. eCollection 2018 Apr.
Focal tumour boosting is currently explored in radiotherapy of prostate cancer to increase tumour control. In this study we applied dose response models for both tumour control and normal tissue complications to explore the benefit of proton therapy (PT) combined with focal tumour boosting, also when accounting for inter-fractional motion.
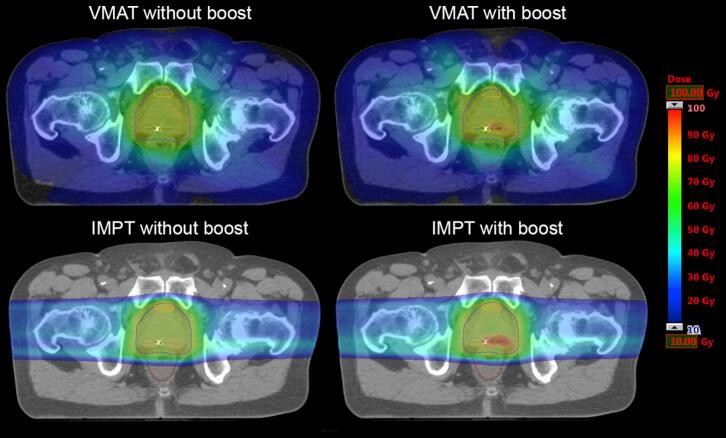
CT scans of seven patients fused with MRI-based index volumes were used. Two volumetric modulated arc therapy (VMAT) plans were created for each patient; one with conventional dose (77 Gy) to the entire prostate, and one with an additional integrated boost (total dose of 95 Gy) to the index lesion. Two corresponding intensity modulated PT (IMPT) plans were created using two lateral opposing spot scanning beams. All plans were evaluated using an MRI-based tumour control probability (TCP) model and normal tissue complication probability (NTCP) models for the rectum and bladder. Plan robustness was evaluated using dose re-calculations on repeat cone-beam CTs.
Across all plans, median TCP increased from 86% (range: 59-98%) without boost to 97% (range: 96-99%) with boost. IMPT plans had lower rectum NTCPs (e.g. 3% vs. 4% for boost plans) but higher bladder NTCPs (20% vs. 18% for boost plans), yet only the bladder NTCPs remained different in the cone beam CT-based re-calculations.
Focal tumour boosting can be delivered with either VMAT or protons, and increases the predicted TCP. The small benefit of IMPT when assessing the planned dose distributions was lost when accounting for inter-fractional motion.
目前在前列腺癌放疗中探索局部肿瘤增敏以提高肿瘤控制率。在本研究中,我们应用肿瘤控制和正常组织并发症的剂量反应模型,探讨质子治疗(PT)联合局部肿瘤增敏的益处,同时考虑分次间运动。
使用7例患者的CT扫描图像与基于MRI的索引体积进行融合。为每位患者创建两个容积调强弧形治疗(VMAT)计划;一个对整个前列腺给予常规剂量(77 Gy),另一个对索引病变额外给予整合增敏(总剂量95 Gy)。使用两个侧向相对的点扫描束创建两个相应的调强质子治疗(IMPT)计划。所有计划均使用基于MRI的肿瘤控制概率(TCP)模型以及直肠和膀胱的正常组织并发症概率(NTCP)模型进行评估。通过在重复锥形束CT上重新计算剂量来评估计划的稳健性。
在所有计划中,中位TCP从无增敏时的86%(范围:59 - 98%)增加到有增敏时的97%(范围:96 - 99%)。IMPT计划的直肠NTCP较低(例如,增敏计划分别为3%和4%),但膀胱NTCP较高(增敏计划分别为20%和18%),然而在基于锥形束CT的重新计算中,只有膀胱的NTCP仍存在差异。
局部肿瘤增敏可通过VMAT或质子治疗实现,并提高预测的TCP。在考虑分次间运动时,评估计划剂量分布时IMPT的微小益处消失。