Surial Bernard, Bertholet Nicolas, Daeppen Jean-Bernard, Darling Katharine E A, Calmy Alexandra, Günthard Huldrych F, Stöckle Marcel, Bernasconi Enos, Schmid Patrick, Rauch Andri, Furrer Hansjakob, Wandeler Gilles
Department of Infectious Diseases, Inselspital, Bern University Hospital, University of Bern, 3010 Bern, Switzerland.
Addiction Medicine, Department of Psychiatry, Lausanne University Hospital, University of Lausanne, 1011 Lausanne, Switzerland.
J Clin Med. 2021 Jan 14;10(2):295. doi: 10.3390/jcm10020295.
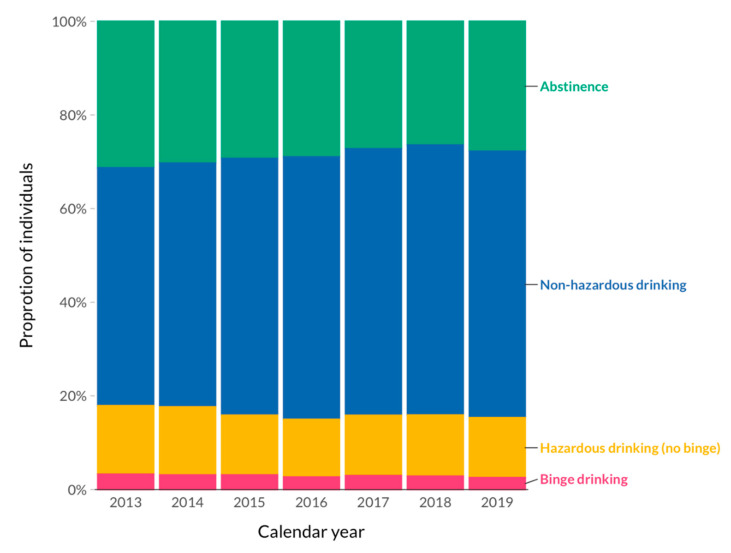
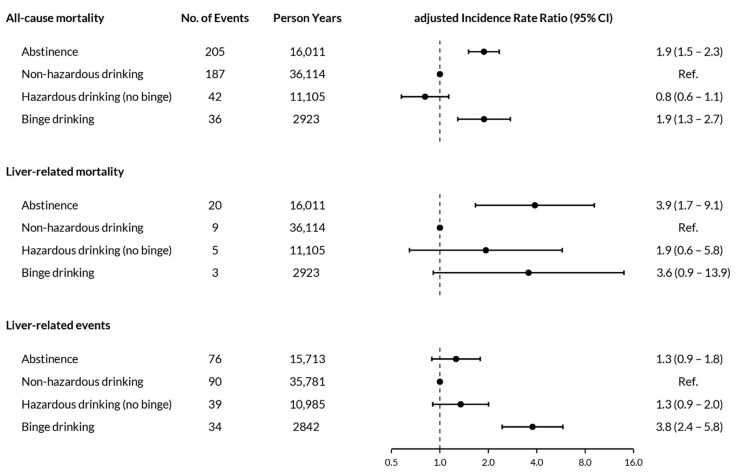
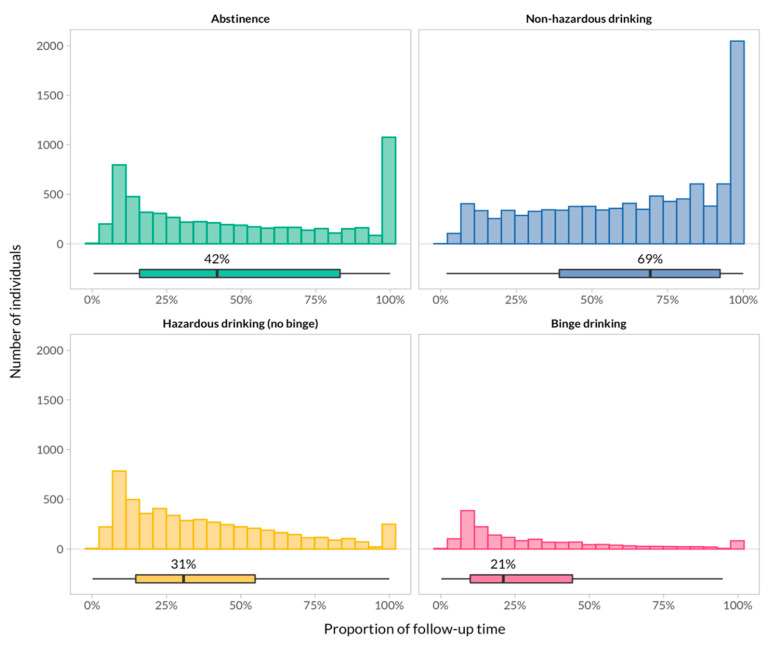
Whereas excessive alcohol consumption increases liver disease incidence and mortality, evidence on the risk associated with specific drinking patterns is emerging. We assessed the impact of binge drinking on mortality and liver disease in the Swiss HIV Cohort Study. All participants with follow-up between 2013 and 2020 were categorized into one of four drinking pattern groups: "abstinence", "non-hazardous drinking", "hazardous but not binge drinking" (Alcohol Use Disorder Identification Test Consumption [AUDIT-C] score ≥ 3 in women and ≥4 in men), and "binge drinking" (≥6 drinks/occasion more than monthly). We estimated adjusted incidence rate ratios (aIRR) for all-cause mortality, liver-related mortality and liver-related events using multivariable quasi-Poisson regression. Among 11,849 individuals (median follow-up 6.8 years), 470 died (incidence rate 7.1/1000 person-years, 95% confidence interval [CI] 6.5-7.8), 37 experienced a liver-related death (0.6/1000, 0.4-0.8), and 239 liver-related events occurred (3.7/1000, 3.2-4.2). Compared to individuals with non-hazardous drinking, those reporting binge drinking were more likely to die (all-cause mortality: aIRR 1.9, 95% CI 1.3-2.7; liver-related mortality: 3.6, 0.9-13.9) and to experience a liver-related event (3.8, 2.4-5.8). We observed no difference in outcomes between participants reporting non-hazardous and hazardous without binge drinking. These findings highlight the importance of assessing drinking patterns in clinical routine.
尽管过量饮酒会增加肝脏疾病的发病率和死亡率,但与特定饮酒模式相关风险的证据正在不断涌现。我们在瑞士HIV队列研究中评估了暴饮对死亡率和肝脏疾病的影响。对2013年至2020年期间有随访记录的所有参与者进行分类,分为四种饮酒模式组之一:“戒酒”、“无危害饮酒”、“有危害但非暴饮”(女性酒精使用障碍识别测试饮酒量 [AUDIT-C] 评分≥3,男性≥4)和“暴饮”(每月超过一次,每次≥6杯)。我们使用多变量准泊松回归估计全因死亡率、肝脏相关死亡率和肝脏相关事件的调整发病率比(aIRR)。在11,849名个体(中位随访6.8年)中,470人死亡(发病率7.1/1000人年,95%置信区间 [CI] 6.5 - 7.8),37人发生肝脏相关死亡(0.6/1000,0.4 - 0.8),239例发生肝脏相关事件(3.7/1000,3.2 - 4.2)。与无危害饮酒者相比,报告有暴饮行为的人更有可能死亡(全因死亡率:aIRR 1.9,95% CI 1.3 - 2.7;肝脏相关死亡率:3.6,0.9 - 13.9)以及发生肝脏相关事件(3.8,2.4 - 5.8)。我们观察到报告无危害饮酒和有危害但无暴饮行为的参与者之间在结局方面没有差异。这些发现凸显了在临床常规中评估饮酒模式的重要性。