Department of Clinical Sciences, Neurosciences, Umeå University, Umea, Sweden.
J Neurol. 2021 Jun;268(6):2161-2168. doi: 10.1007/s00415-021-10399-8. Epub 2021 Jan 21.
Rituximab is safe and effective for treating relapsing-remitting multiple sclerosis (RRMS) according to phase II and observational studies. There are limited data on disease activity after discontinuation and dose reduction. The objective of this study was to evaluate the effects on inflammatory disease activity after discontinuation or dose reduction of rituximab in patients with RRMS or clinically isolated syndrome (CIS).
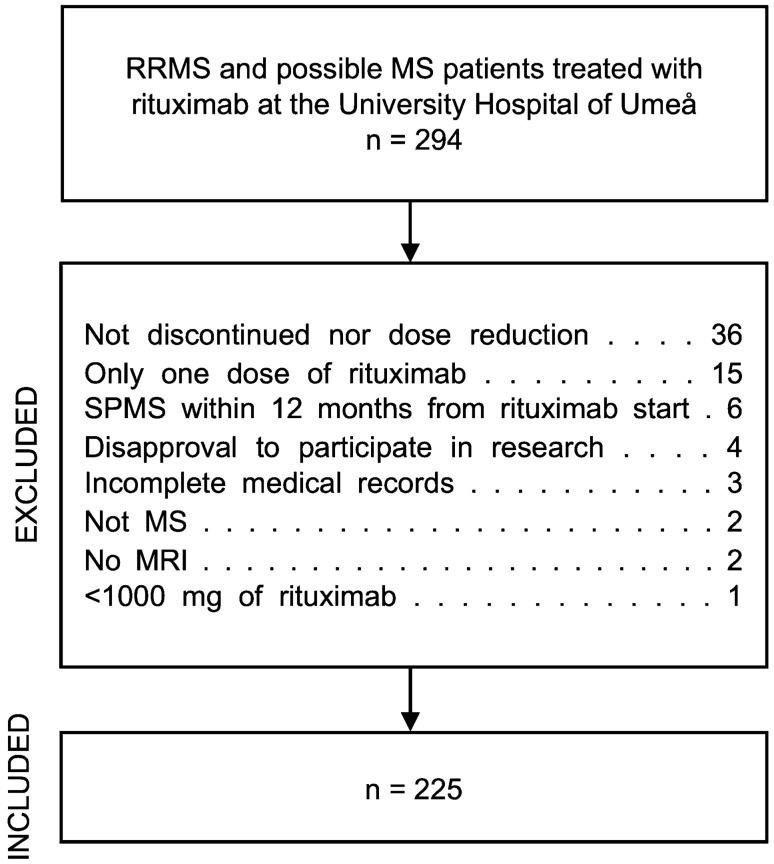
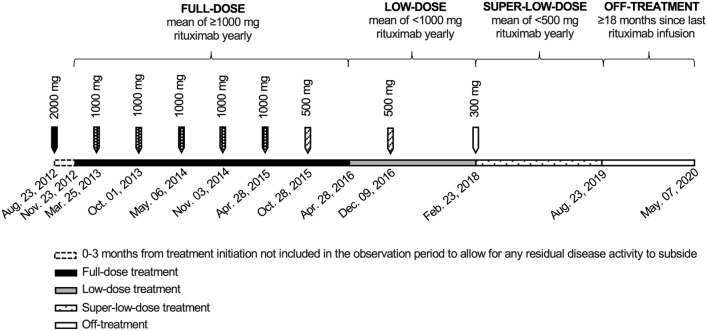
In this retrospective observational study, we included all RRMS and CIS patients ever treated with rituximab at the University Hospital of Umeå who had either; (1) discontinued treatment at any time or (2) reduced the dose to a mean of < 1000 mg yearly. The patients served as their own controls by contributing patient years on full dose, reduced dose, and off treatment.
A total of 225 patients treated with mean (SD) 6256 (2456) mg rituximab during mean (SD) 6.5 (2.0) years were included. There were no differences regarding the annualized relapse rates during full dose versus reduced dose or off treatment (0.02 versus < 0.01 and 0.02, p = 0.09), neither regarding proportion MRI scans with new or enlarged T2 lesions (0.03 versus 0.01 and 0.03, p = 0.37) or contrast-enhancing lesions (< 0.01 versus 0 and 0.02, p = 0.22).
This study indicates that rituximab has long-term effects on inflammatory disease activity and that disease reactivation is rare in MS patients who discontinued treatment for any reason. It also suggests that treatment with low-dose rituximab (< 1000 mg yearly) is sufficient to maintain suppression of inflammatory disease activity in patients with stable disease.
利妥昔单抗在治疗复发缓解型多发性硬化症(RRMS)方面是安全有效的,这一结论基于 II 期和观察性研究。关于停药和剂量减少后疾病活动的相关数据有限。本研究的目的是评估 RRMS 或临床孤立综合征(CIS)患者停药或减少利妥昔单抗剂量后对炎症性疾病活动的影响。
本回顾性观察性研究纳入了所有在瑞典于默奥大学医院接受过利妥昔单抗治疗的 RRMS 和 CIS 患者,他们要么:(1)在任何时候停药;(2)将剂量减少至平均每年<1000 毫克。患者以自身为对照,分别贡献全剂量、低剂量和停药的患者年数。
共纳入 225 例患者,平均(标准差)接受利妥昔单抗 6256(2456)毫克,平均(标准差)治疗 6.5(2.0)年。全剂量与低剂量或停药时的年复发率无差异(0.02 与<0.01 和 0.02,p=0.09),MRI 扫描显示新或扩大 T2 病变的比例也无差异(0.03 与 0.01 和 0.03,p=0.37)或对比增强病变(<0.01 与 0 和 0.02,p=0.22)。
本研究表明利妥昔单抗对炎症性疾病活动具有长期影响,且 MS 患者无论出于何种原因停药,疾病复发均罕见。这也表明,低剂量利妥昔单抗(<1000 毫克/年)治疗足以维持疾病稳定患者炎症性疾病活动的抑制。