Center for Cardiac Arrest Prevention, Smidt Heart Institute, Cedars-Sinai Health System, Los Angeles, California, USA.
Ventura County Emergency Medical Services, Ventura, California, USA.
JACC Clin Electrophysiol. 2021 Jan;7(1):6-11. doi: 10.1016/j.jacep.2020.08.010. Epub 2020 Aug 14.
The purpose of this study was to evaluate the potential impact of the coronavirus disease-2019 (COVID-19) pandemic on out-of-hospital cardiac arrest (OHCA) responses and outcomes in 2 U.S. communities with relatively low infection rates.
Studies in areas with high COVID-19 infection rates indicate that the pandemic has had direct and indirect effects on community responses to OHCA and negative impacts on survival. Data from areas with lower infection rates are lacking.
Cases of OHCA in Multnomah County, Oregon, and Ventura County, California, with attempted resuscitation by emergency medical services (EMS) from March 1 to May 31, 2020, and from March 1 to May 31, 2019, were evaluated.
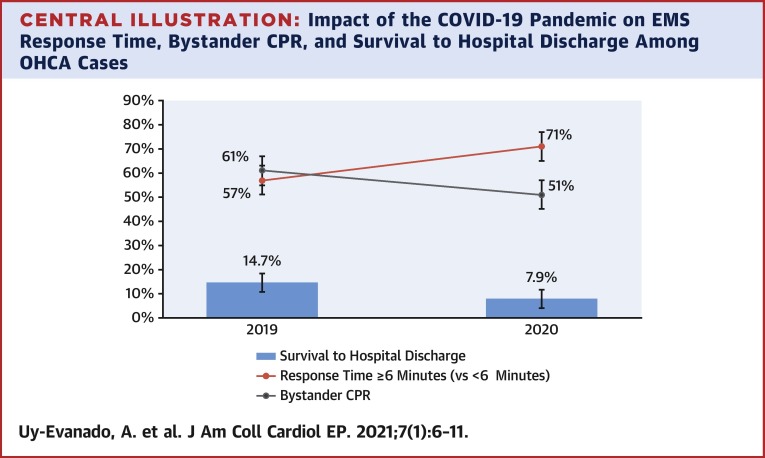
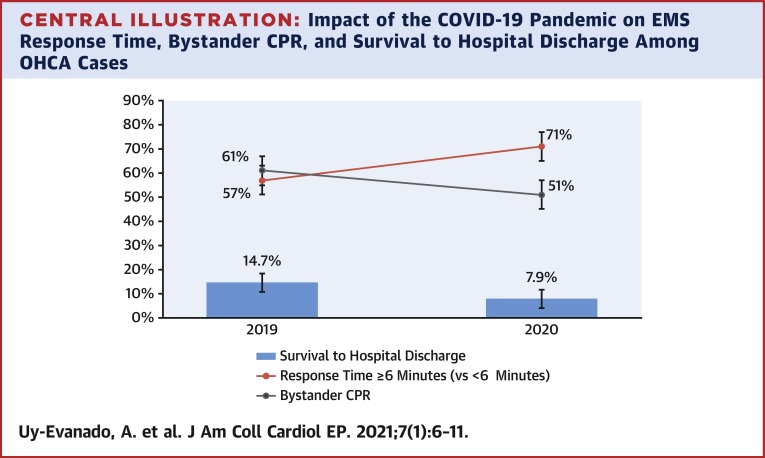
In a comparison of 231 OHCA in 2019 to 278 in 2020, the proportion of cases receiving bystander cardiopulmonary resuscitation (CPR) was lower in 2020 (61% to 51%, respectively; p = 0.02), and bystander use of automated external defibrillators (AEDs) declined (5% to 1%, respectively; p = 0.02). EMS response time increased (6.6 ± 2.0 min to 7.6 ± 3.0 min, respectively; p < 0.001), and fewer OHCA cases survived to hospital discharge (14.7% to 7.9%, respectively; p = 0.02). Incidence rates did not change significantly (p > 0.07), and coronavirus infection rates were low (Multnomah County, 143/100,000; Ventura County, 127/100,000 as of May 31) compared to rates of ∼1,600 to 3,000/100,000 in the New York City region at that time.
The community response to OHCA was altered from March to May 2020, with less bystander CPR, delays in EMS response time, and reduced survival from OHCA. These results highlight the pandemic's indirect negative impact on OHCA, even in communities with relatively low incidence of COVID-19 infection, and point to potential opportunities for countering the impact.
本研究旨在评估 2019 年冠状病毒病(COVID-19)大流行对美国两个社区院外心脏骤停(OHCA)反应和结局的潜在影响,这两个社区的感染率相对较低。
在感染率较高的地区进行的研究表明,大流行对社区对 OHCA 的反应产生了直接和间接影响,并对生存率产生了负面影响。在感染率较低的地区缺乏相关数据。
评估了俄勒冈州 Multnomah 县和加利福尼亚州 Ventura 县的 OHCA 病例,这些病例在 2020 年 3 月 1 日至 5 月 31 日和 2019 年 3 月 1 日至 5 月 31 日期间由急救医疗服务(EMS)进行了尝试复苏。
在 2019 年的 231 例 OHCA 与 2020 年的 278 例 OHCA 比较中,2020 年接受旁观者心肺复苏术(CPR)的病例比例较低(分别为 61%和 51%;p=0.02),旁观者使用自动体外除颤器(AED)的比例下降(分别为 5%和 1%;p=0.02)。EMS 反应时间延长(分别为 6.6±2.0 分钟和 7.6±3.0 分钟;p<0.001),更少的 OHCA 病例存活至出院(分别为 14.7%和 7.9%;p=0.02)。发病率没有显著变化(p>0.07),冠状病毒感染率较低(截至 5 月 31 日,Multnomah 县为 143/100,000;Ventura 县为 127/100,000),而当时纽约市地区的发病率约为 1600 至 3000/100,000。
2020 年 3 月至 5 月,OHCA 的社区反应发生了变化,旁观者 CPR 减少,EMS 反应时间延迟,OHCA 患者的存活率降低。这些结果强调了大流行对 OHCA 的间接负面影响,即使在 COVID-19 感染率相对较低的社区也是如此,并指出了对抗这种影响的潜在机会。