Department of Hematology, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, No. 3 Qingchun East Rd., Hangzhou, 310016, Zhejiang Province, People's Republic of China.
Sci Rep. 2021 Jan 22;11(1):2125. doi: 10.1038/s41598-020-80724-0.
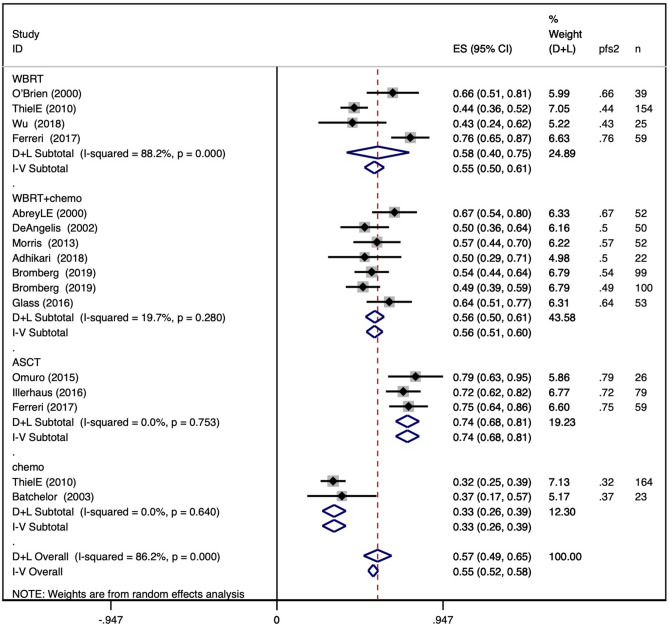
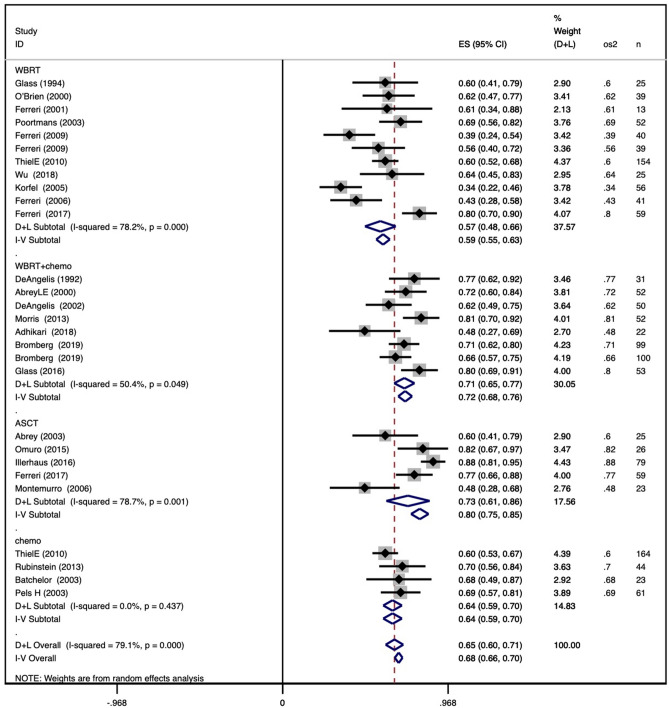
With the exception of high-dose methotrexate (HD-MTX), there is currently no defined standard treatment for newly diagnosed primary central nervous system lymphoma (PCNSL). This review focused on first-line induction and consolidation treatment of PCNSL and aimed to determine the optimal combination of HD-MTX and the long-term beneficial consolidation methods. A comprehensive literature search of MEDLINE identified 1407 studies, among which 31 studies met the inclusion criteria. The meta-analysis was performed by using Stata SE version 15. Forest plots were generated to report combined outcomes like the complete response rate (CRR), overall survival, and progression-free survival. We also conducted univariate regression analyses of the baseline characteristics to identify the source of heterogeneity. Pooled analysis showed a CRR of 41% across all HD-MTX-based regimens, and three- and four-drug regimens had better CRRs than HD-MTX monotherapy. In all combinations based on HD-MTX, the HD-MTX + procarbazine + vincristine (MPV) regimen showed pooled CRRs of 63% and 58% with and without rituximab, respectively, followed by the rituximab + HD-MTX + temozolomide regimen, which showed a pooled CRR of 60%. Pooled PFS and OS showed that post-remission consolidation with autologous stem cell transplantation (ASCT) was associated with the best survival outcome, with a pooled 2-year OS of 80%, a 2-year PFS of 74%, a 5-year OS of 77%, and a 5-year PFS of 63%. Next, whole-brain radiation therapy (WBRT) + chemotherapy showed a pooled 2-year OS of 72%, 2-year PFS of 56%, 5-year OS of 55%, and 5-year PFS of 41%, with no detectable CR heterogeneity throughout the entire treatment process. In HD-MTX-based therapy of newly diagnosed PCNSL, MPV with or without rituximab can be chosen as the inductive regimen, and the rituximab + HD-MTX + temozolomide regimen is also a practical choice. Based on our study, high-dose chemotherapy supported by ASCT is an efficacious approach for consolidation. Consolidation with WBRT + chemotherapy can be another feasible approach.
除了大剂量甲氨蝶呤(HD-MTX)外,目前尚无明确的新诊断原发性中枢神经系统淋巴瘤(PCNSL)标准治疗方法。本综述重点关注 PCNSL 的一线诱导和巩固治疗,并旨在确定 HD-MTX 与长期有益的巩固方法的最佳组合。通过对 MEDLINE 进行全面文献检索,确定了 1407 项研究,其中 31 项研究符合纳入标准。使用 Stata SE 版本 15 进行了荟萃分析。生成森林图以报告联合结局,如完全缓解率(CRR)、总生存率和无进展生存率。我们还对基线特征进行了单变量回归分析,以确定异质性的来源。汇总分析显示,所有基于 HD-MTX 的方案的 CRR 为 41%,三药和四药方案的 CRR 优于 HD-MTX 单药治疗。在所有基于 HD-MTX 的组合中,HD-MTX+丙卡巴肼+长春新碱(MPV)方案在有和没有利妥昔单抗的情况下,分别显示出 63%和 58%的汇总 CRR,其次是利妥昔单抗+HD-MTX+替莫唑胺方案,其显示出 60%的汇总 CRR。汇总的 PFS 和 OS 显示,缓解后自体干细胞移植(ASCT)巩固治疗与最佳生存结局相关,2 年 OS 为 80%,2 年 PFS 为 74%,5 年 OS 为 77%,5 年 PFS 为 63%。接下来,全脑放疗(WBRT)+化疗显示出 2 年 OS 为 72%、2 年 PFS 为 56%、5 年 OS 为 55%、5 年 PFS 为 41%,整个治疗过程中未检测到 CR 异质性。在新诊断的 PCNSL 的 HD-MTX 治疗中,可以选择 MPV 加或不加利妥昔单抗作为诱导方案,利妥昔单抗+HD-MTX+替莫唑胺方案也是一种实用的选择。根据我们的研究,ASCT 支持的大剂量化疗是巩固治疗的有效方法。WBRT+化疗巩固治疗也是一种可行的方法。