Department of Digestive Surgery, Breast and Thyroid Surgery, Kagoshima University Graduate School of Medical and Dental Sciences, 8-35-1 Sakuragaoka, Kagoshima, 890-8520, Japan.
Department of Onco-biological Surgery, Kagoshima University Graduate School of Medical and Dental Sciences, Kagoshima, Japan.
BMC Cancer. 2021 Jan 23;21(1):95. doi: 10.1186/s12885-021-07801-z.
Postoperative complications have been linked to the morbidity and mortality of several cancers. However, predicting whether complications will occur in the early period after surgery or not is challenging. Hence, this study aimed to examine the diagnostic accuracy of serum creatine phosphokinase (CPK) and c-reactive protein (CRP) in predicting the development of postgastrectomy complications.
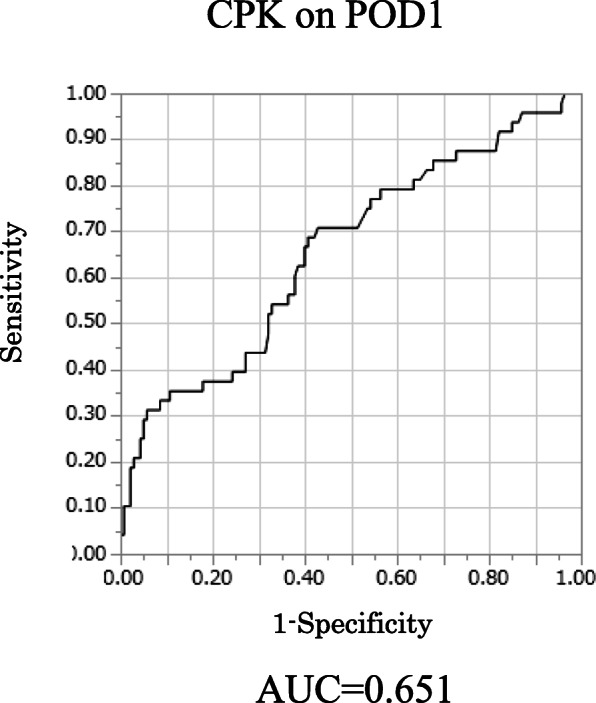
We retrospectively analyzed 188 patients with gastric cancer (GC) who underwent gastrectomy. The diagnostic accuracy of serum CPK and CRP was investigated using the areas under the curves (AUC). The CPK ratio was defined as the CPK on postoperative day (POD) 1 to the CPK on a preoperative day.
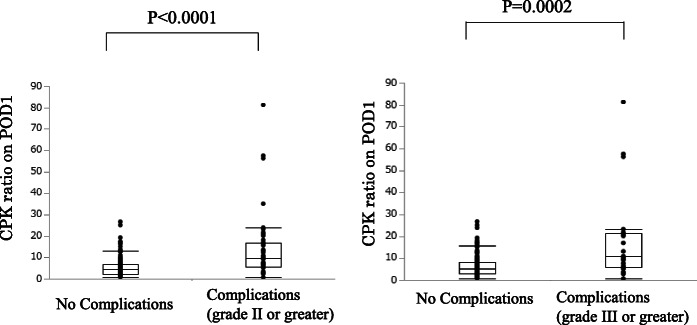
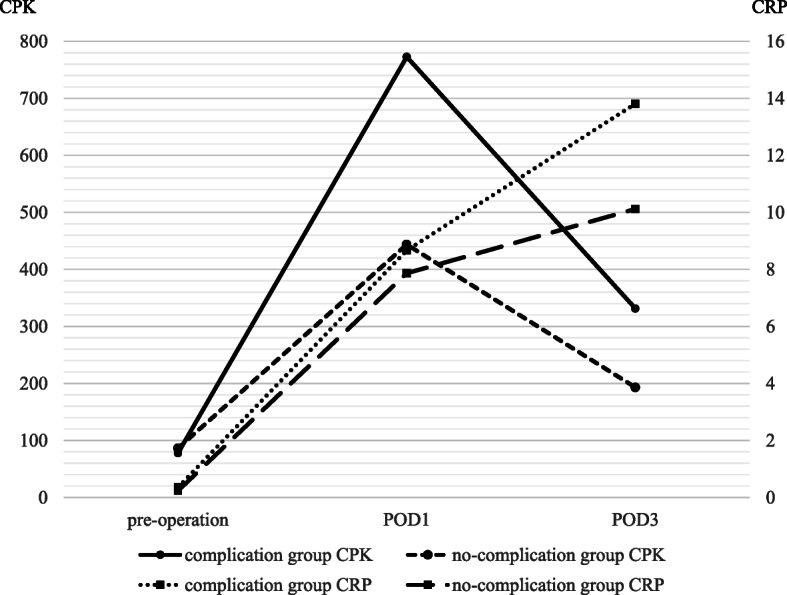
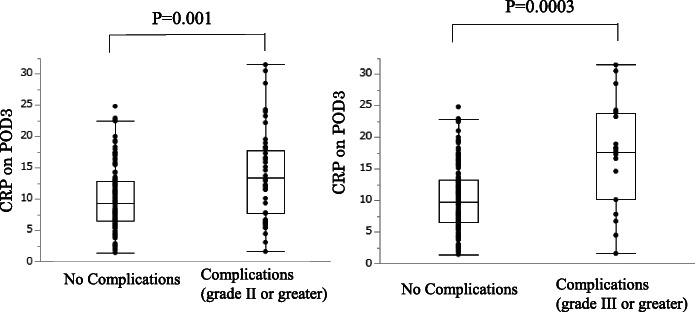
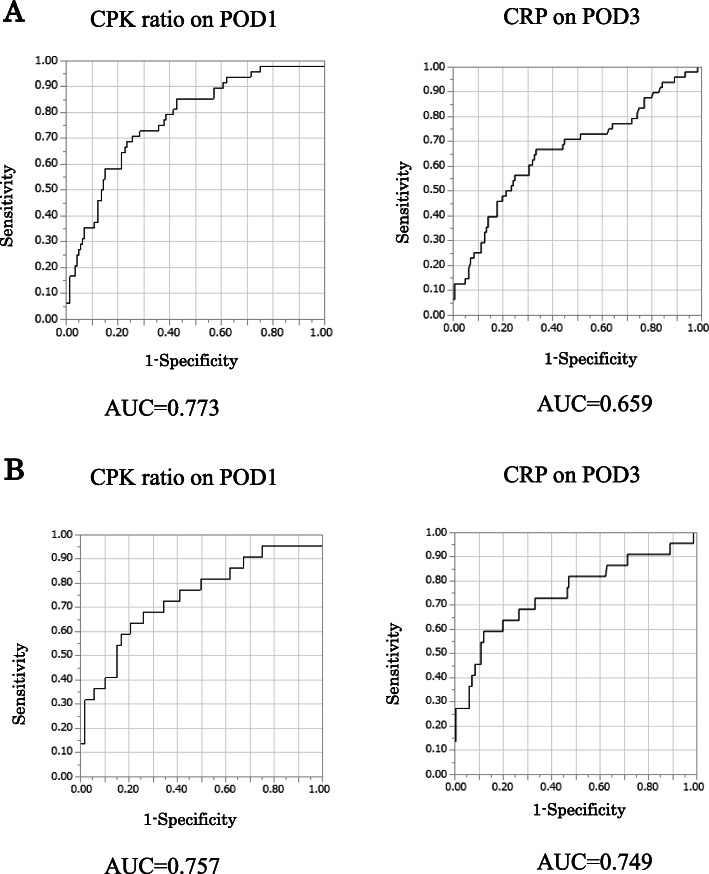
Out of 188 patients, 48 (25.5%) developed postoperative complications. The complications group had a greater operative time (p = 0.037), higher CPK ratio on POD1 (p < 0.0001), and a higher serum CRP level on POD3 (p = 0.001). The AUC for the CPK ratio was 0.772, with an optimal cutoff value of 7.05, whereas that for CRP was 0.659, with an optimal cutoff value of 11.4 mg/L. The CPK ratio on POD1 (p < 0.0001) and the CRP on POD3 (p = 0.007) were independent factors for predicting the development of postgastrectomy complications. The CPK ratio on POD1 and the CRP on POD3 predicted postgastrectomy complications in 41 patients (85.4%). According to combined value of both CPK ratio and CRP level, the positive predictive value and the negative predictive value was 0.70 and 0.829. And sensitivity and specificity were 0.438 and 0.936.
The CPK ratio on POD1 and the CRP on POD3 after gastrectomy for GC were predictive factors for complication development and may be employed to prevent the development of such complications and improve the prognosis of patients with GC.
术后并发症与多种癌症的发病率和死亡率有关。然而,预测手术后早期是否会发生并发症具有挑战性。因此,本研究旨在探讨血清肌酸磷酸激酶(CPK)和 C 反应蛋白(CRP)在预测胃切除术后并发症发展中的诊断准确性。
我们回顾性分析了 188 例接受胃癌(GC)胃切除术的患者。使用曲线下面积(AUC)来研究血清 CPK 和 CRP 的诊断准确性。CPK 比值定义为术后第 1 天(POD1)的 CPK 与术前 1 天的 CPK 之比。
188 例患者中,48 例(25.5%)发生术后并发症。并发症组的手术时间更长(p=0.037),POD1 的 CPK 比值更高(p<0.0001),POD3 的血清 CRP 水平更高(p=0.001)。CPK 比值的 AUC 为 0.772,最佳截断值为 7.05,而 CRP 的 AUC 为 0.659,最佳截断值为 11.4mg/L。POD1 的 CPK 比值(p<0.0001)和 POD3 的 CRP(p=0.007)是预测胃切除术后并发症发展的独立因素。POD1 的 CPK 比值和 POD3 的 CRP 预测了 41 例(85.4%)胃切除术后并发症。根据 CPK 比值和 CRP 水平的联合值,阳性预测值和阴性预测值分别为 0.70 和 0.829。灵敏度和特异性分别为 0.438 和 0.936。
GC 胃切除术后 POD1 的 CPK 比值和 POD3 的 CRP 是并发症发展的预测因素,可用于预防并发症的发生,改善 GC 患者的预后。