Division of Cardiac Surgery, Department of Surgery, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, Alberta, Canada.
Division of Cardiothoracic Surgery, Al Azhar University, Cairo, Egypt.
Syst Rev. 2021 Jan 23;10(1):36. doi: 10.1186/s13643-021-01579-8.
Preoperative anemia is a common comorbidity that often necessitates allogeneic blood transfusion (ABT). As there is a risk associated with blood transfusions, preoperative intravenous iron (IV) has been proposed to increase the hemoglobin to reduce perioperative transfusion; however, randomized controlled trials (RCT) investigating this efficacy for IV iron are small, limited, and inconclusive. Consequently, a meta-analysis that pools these studies may provide new and clinically useful information.
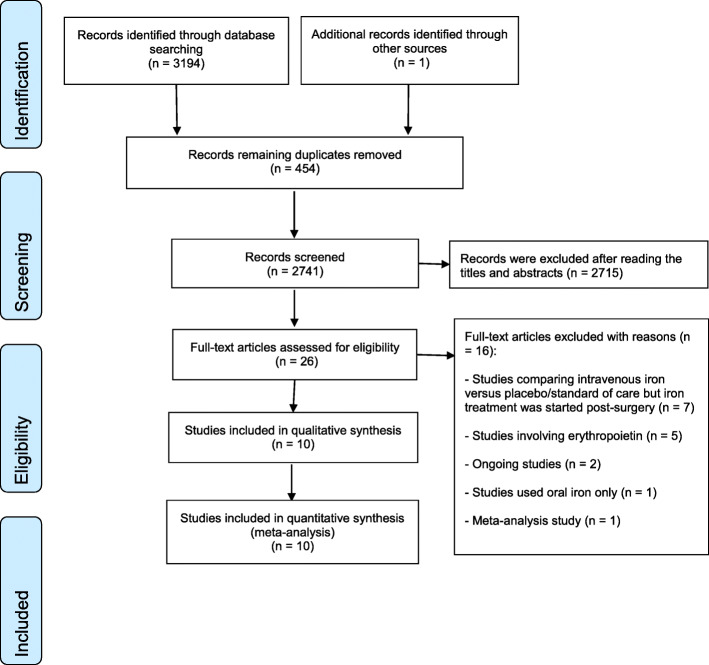
METHODS/DESIGN: Databases of MEDLINE, EMBASE, EBM Reviews; Cochrane-controlled trial registry; Scopus; registries of health technology assessment and clinical trials; Web of Science; ProQuest Dissertations and Theses; Clinicaltrials.gov; and Conference Proceedings Citation Index-Science (CPCI-S) were searched. Also, we screened all the retrieved reference lists.
Titles and abstracts were screened for relevance (i.e., relevant, irrelevant, or potentially relevant). Then, we screened full texts of those citations identified as potentially applicable.
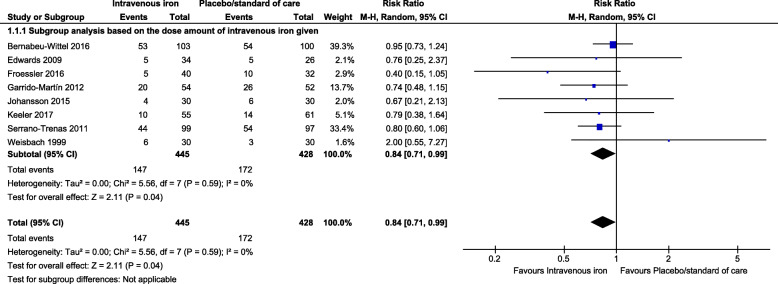
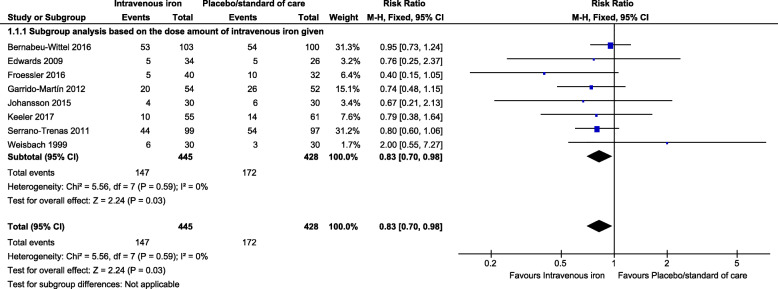
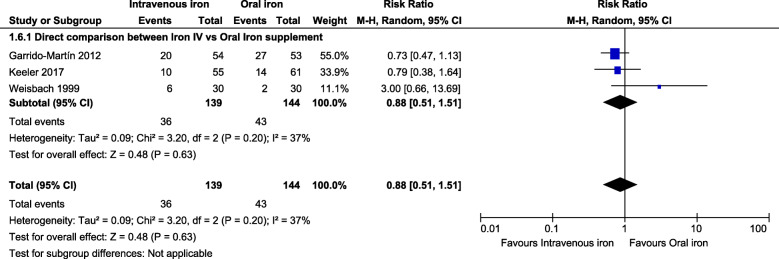
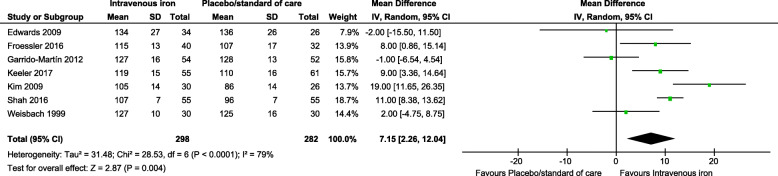
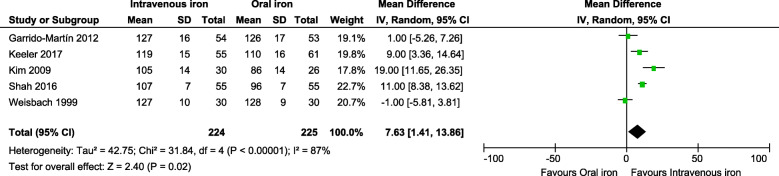
Our search found 3195 citations and ten RCTs (1039 participants) that met our inclusion criteria. Preoperative IV iron supplementation significantly decreases ABT by 16% (risk ratio (RR): 0.84, 95% confidence interval [CI]: 0.71, 0.99, p = 0.04). In addition, preoperatively, hemoglobin levels increased after receiving IV iron (mean difference [MD] between the study groups: 7.15 g/L, 95% CI: 2.26, 12.04 g/L, p = 0.004) and at follow-up > 4 weeks postoperatively (MD: 6.46 g/L, 95% CI: 3.10, 9.81, p = 0.0002). Iron injection was not associated with increased incidence of non-serious or serious adverse effects across groups (RR: 1.13, 95% CI: 0.78, 1.65, p = 0.52) and (RR: 0.96, 95% CI: 0.44, 2.10, p = 0.92) respectively.
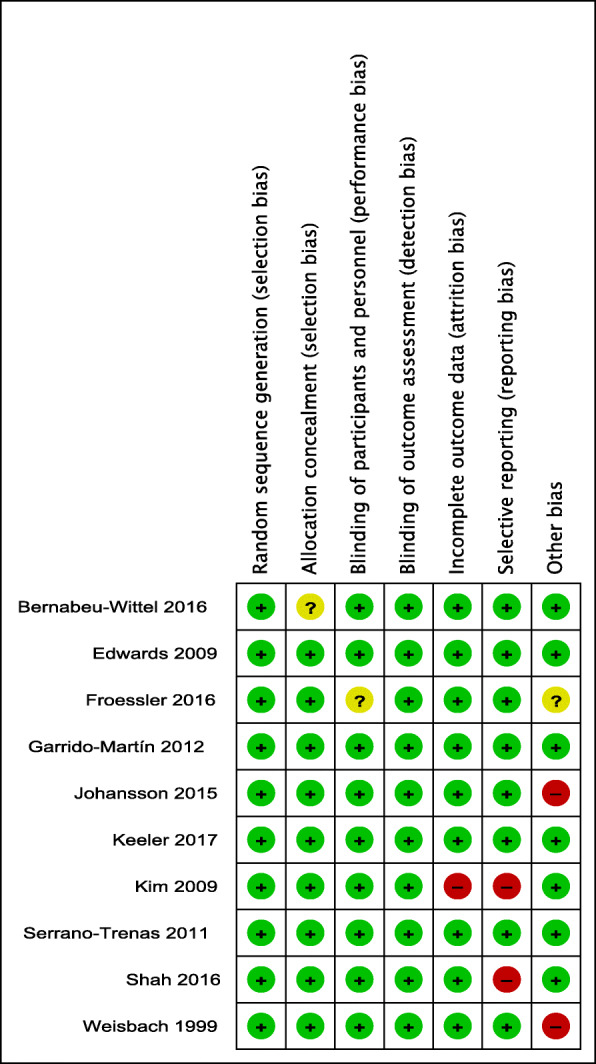
With moderate certainty, due to the high risk of bias in some studies in one or two domains, we found intravenous iron supplementation is associated with a significant decrease in the blood transfusions rate, and modest hemoglobin concentrations rise when injected pre-surgery compared with placebo or oral iron supplementation. However, further full-scale randomized controlled trials with robust methodology are required. In particular, the safety, quality of life, and cost-effectiveness of different intravenous iron preparations require further evaluation.
术前贫血是一种常见的合并症,常需要异体输血(ABT)。由于输血存在风险,因此已提出术前静脉内铁(IV)治疗以增加血红蛋白以减少围手术期输血;然而,针对 IV 铁治疗这种疗效的随机对照试验(RCT)规模较小、有限且不一致。因此,汇总这些研究的荟萃分析可能会提供新的且具有临床意义的信息。
方法/设计:检索 MEDLINE、EMBASE、EBM 评价数据库; Cochrane 对照试验注册中心;Scopus;卫生技术评估和临床试验登记处;Web of Science;ProQuest 论文和论文;Clinicaltrials.gov;以及 Conference Proceedings Citation Index-Science(CPCI-S)。此外,我们还筛选了所有检索到的参考文献列表。
筛选标题和摘要以确定相关性(即相关、不相关或可能相关)。然后,我们筛选了那些被确定为可能适用的引文的全文。
我们的搜索发现了 3195 条引文和 10 项 RCT(1039 名参与者)符合纳入标准。术前 IV 铁补充剂可显著降低 ABT 率 16%(风险比(RR):0.84,95%置信区间 [CI]:0.71,0.99,p = 0.04)。此外,术前接受 IV 铁治疗后血红蛋白水平升高(研究组间平均差异[MD]:7.15 g/L,95% CI:2.26,12.04 g/L,p = 0.004),且在术后> 4 周随访时仍升高(MD:6.46 g/L,95% CI:3.10,9.81,p = 0.0002)。各组之间铁注射与非严重或严重不良事件的发生率增加无关(RR:1.13,95% CI:0.78,1.65,p = 0.52)和(RR:0.96,95% CI:0.44,2.10,p = 0.92)。
由于一些研究在一个或两个领域存在高偏倚风险,因此我们有中等确定性,发现与安慰剂或口服铁补充剂相比,静脉内铁补充剂与显著降低输血率相关,且术前注射后血红蛋白浓度适度升高。然而,需要进一步进行具有稳健方法学的大规模随机对照试验。特别是,不同静脉内铁制剂的安全性、生活质量和成本效益需要进一步评估。