Medication Outcomes Center, Department of Clinical Pharmacy, University of California, San Francisco School of Pharmacy, San Francisco, California.
Division of Infectious Diseases, Department of Medicine, Oregon Health and Sciences University School of Medicine, Portland, Oregon.
Infect Control Hosp Epidemiol. 2021 Sep;42(9):1090-1097. doi: 10.1017/ice.2020.1368. Epub 2021 Jan 25.
To evaluate broad-spectrum intravenous antibiotic use before and after the implementation of a revised febrile neutropenia management algorithm in a population of adults with hematologic malignancies.
Quasi-experimental study.
Patients admitted between 2014 and 2018 to the Adult Malignant Hematology service of an acute-care hospital in the United States.
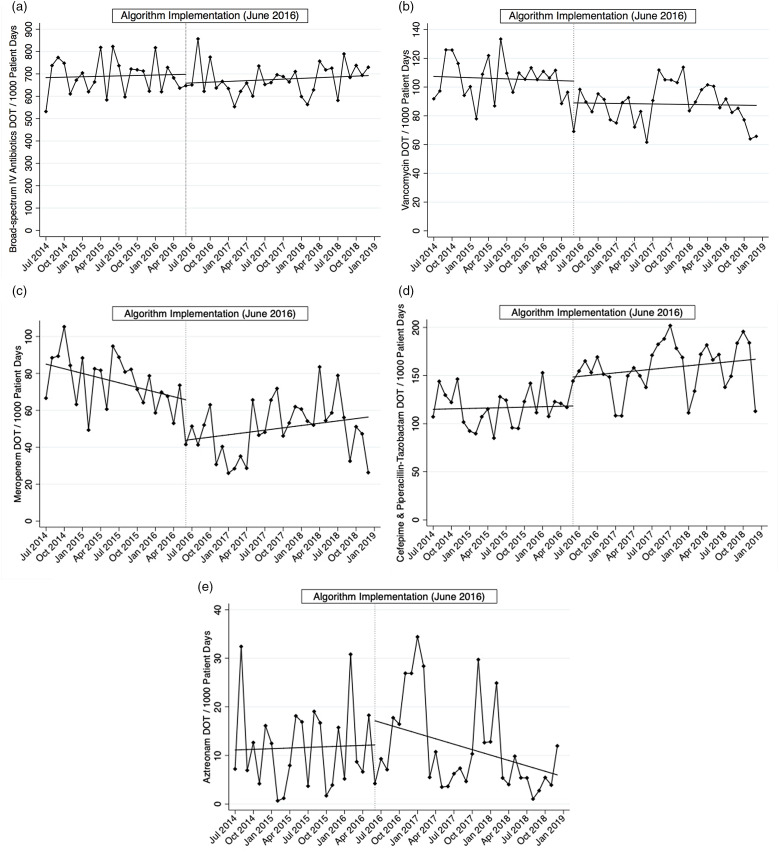
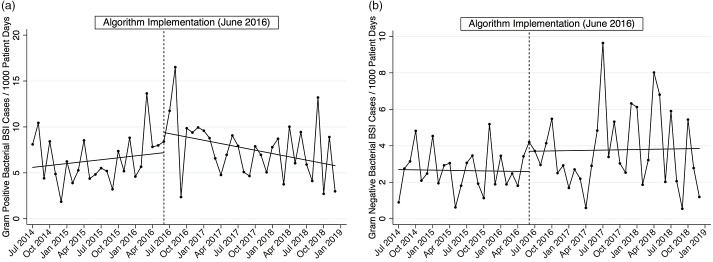
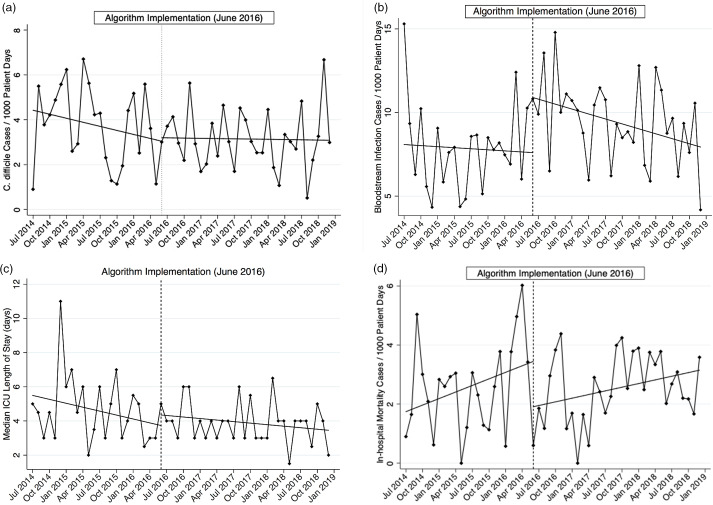
Aggregate data for adult malignant hematology service were obtained for population-level antibiotic use: days of therapy (DOT), C. difficile infections, bacterial bloodstream infections, intensive care unit (ICU) length of stay, and in-hospital mortality. All rates are reported per 1,000 patient days before the implementation of an febrile neutropenia management algorithm (July 2014-May 2016) and after the intervention (June 2016-December 2018). These data were compared using interrupted time series analysis.
In total, 2,014 patients comprised 6,788 encounters and 89,612 patient days during the study period. Broad-spectrum intravenous (IV) antibiotic use decreased by 5.7% with immediate reductions in meropenem and vancomycin use by 22 (P = .02) and 15 (P = .001) DOT per 1,000 patient days, respectively. Bacterial bloodstream infection rates significantly increased following algorithm implementation. No differences were observed in the use of other antibiotics or safety outcomes including C. difficile infection, ICU length of stay, and in-hospital mortality.
Reductions in vancomycin and meropenem were observed following the implementation of a more stringent febrile neutropenia management algorithm, without evidence of adverse outcomes. Successful implementation occurred through a collaborative effort and continues to be a core reinforcement strategy at our institution. Future studies evaluating patient-level data may identify further stewardship opportunities in this population.
评估在修订发热性中性粒细胞减少症管理算法实施前后,血液恶性肿瘤成人患者广谱静脉用抗生素的使用情况。
准实验研究。
美国一家急性护理医院成人恶性血液病科收治的 2014 年至 2018 年期间的患者。
获取成人恶性血液病科的人群水平抗生素使用数据:治疗天数(DOT)、艰难梭菌感染、细菌性血流感染、重症监护病房(ICU)住院时间和院内死亡率。所有比率均按发热性中性粒细胞减少症管理算法实施前(2014 年 7 月至 2016 年 5 月)和干预后(2016 年 6 月至 2018 年 12 月)每 1000 个患者天报告。使用中断时间序列分析比较这些数据。
在研究期间,共有 2014 名患者构成了 6788 次就诊和 89612 个患者天。广谱静脉(IV)抗生素使用减少了 5.7%,其中美罗培南和万古霉素的使用分别减少了 22(P=0.02)和 15(P=0.001)DOT/1000 患者天。细菌性血流感染率在算法实施后显著增加。其他抗生素的使用或安全性结果(包括艰难梭菌感染、ICU 住院时间和院内死亡率)无差异。
在实施更严格的发热性中性粒细胞减少症管理算法后,观察到万古霉素和美罗培南的使用减少,没有不良结果的证据。通过协作努力成功实施,并继续成为我们机构的核心强化策略。未来评估患者水平数据的研究可能会在该人群中发现进一步的管理机会。