Kinnaman Michael D, Zhu Chong, Weiser Daniel A, Mohiuddin Sana, Hingorani Pooja, Roth Michael, Gill Jonathan, Janeway Katherine A, Gorlick Richard, Lessnick Stephen L, Grohar Patrick J
Department of Pediatrics, Memorial Sloan Kettering Cancer Center, New York, NY, USA.
Brii Biosciences, Beijing, China.
Sarcoma. 2020 Dec 5;2020:3498549. doi: 10.1155/2020/3498549. eCollection 2020.
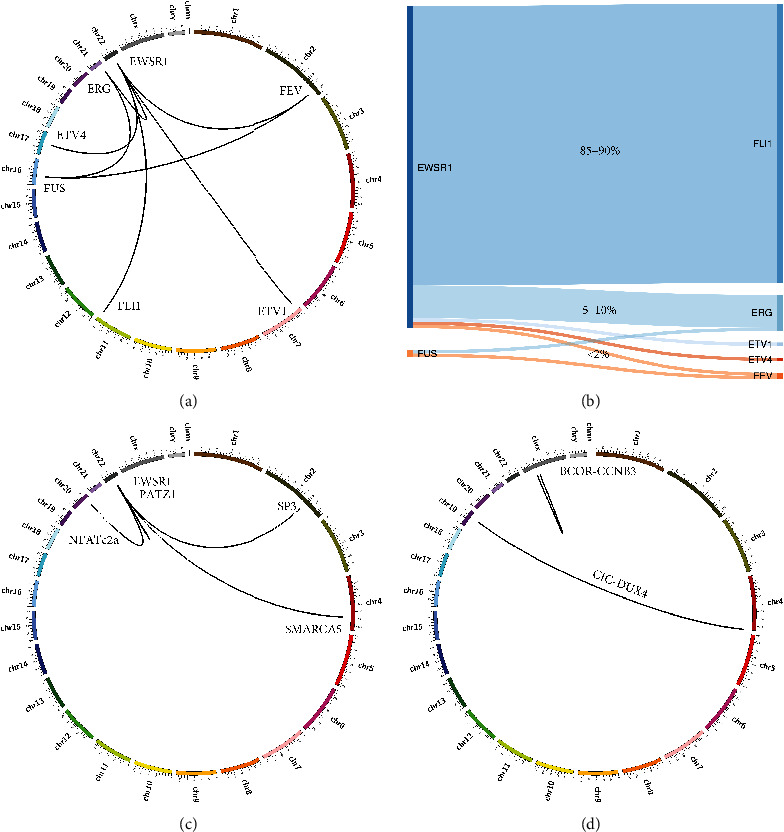
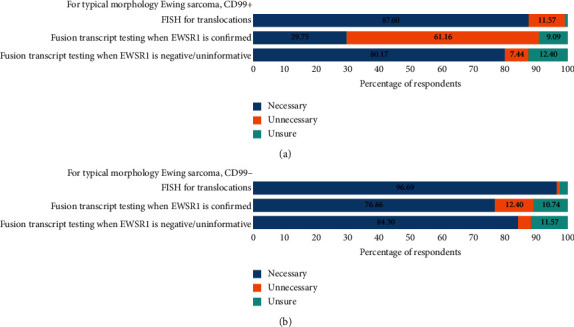
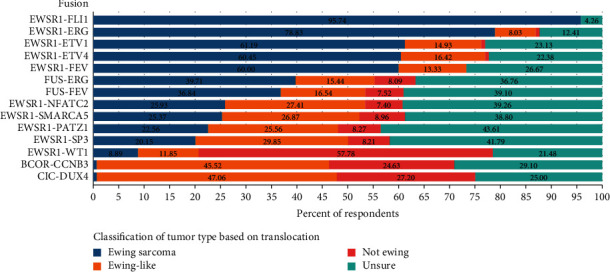
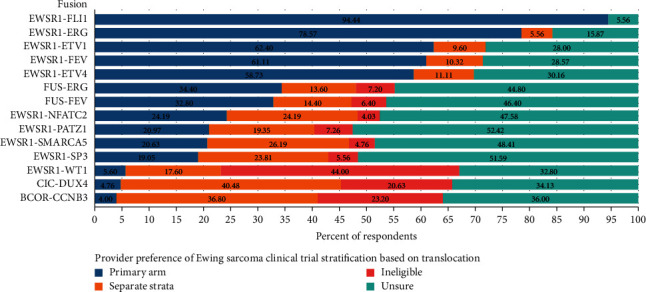
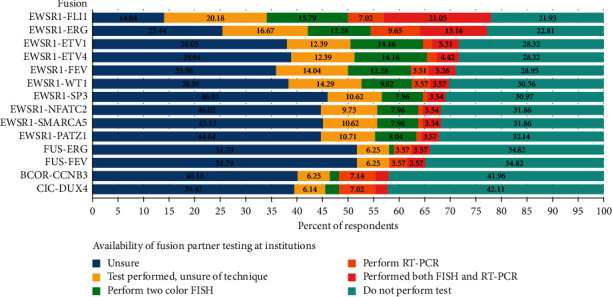
Advances in molecular diagnostics have identified subsets of Ewing and Ewing-like sarcomas driven by variant translocations with unique biology. It is likely that patients with these tumours will have different clinical features and therapeutic outcomes. Nevertheless, the management of these patients both locally and within cooperative group trials depends on the local pathological diagnosis. It is not known what molecular diagnostic approaches are employed by local pathologists or if the exact translocation is commonly determined. In addition, it is not known what therapeutic approaches are employed for these patients or what cooperative trials are deemed appropriate for these patients by expert consensus. To answer these questions, we performed an international survey of oncologists and pathologists to better understand the diagnostic approaches used to identify variant translocations and the influence the findings have on therapy and clinical trial eligibility. An online survey was distributed to oncologists and pathologists primarily in North America. A total of 141 surveys were completed, representing a 28% response rate. The majority of respondents considered EWSR1-ETS gene family translocations (range 61-96%) to be Ewing sarcoma and would include them on the primary arm of a Ewing sarcoma clinical trial. There was a lack of consensus on how to classify and stratify BCOR-CCNB3, CIC-DUX4, and EWSR1+ with non-ETS partner fusions. Most respondents were either unsure how their institution tested, or their institution did not perform the test. In cases with atypical Ewing morphology, most respondents favoured additional fusion transcript testing. There is a lack of consensus regarding the classification and stratification of rare molecular subtypes in Ewing sarcoma. It is not clear how these alternative translocations have impacted outcomes for past clinical studies. This suggests a need for molecular confirmation of diagnoses and centralized or minimum standardization of testing for future trial enrolment.
分子诊断学的进展已经确定了由具有独特生物学特性的变异易位驱动的尤因肉瘤和尤因样肉瘤亚群。这些肿瘤患者可能具有不同的临床特征和治疗结果。然而,这些患者在当地以及合作组试验中的管理取决于当地的病理诊断。目前尚不清楚当地病理学家采用何种分子诊断方法,也不清楚是否通常能确定确切的易位情况。此外,尚不清楚这些患者采用了何种治疗方法,或者专家共识认为哪些合作试验适用于这些患者。为了回答这些问题,我们对肿瘤学家和病理学家进行了一项国际调查,以更好地了解用于识别变异易位的诊断方法以及这些结果对治疗和临床试验资格的影响。一项在线调查主要分发给了北美地区的肿瘤学家和病理学家。共完成了141份调查问卷,回复率为28%。大多数受访者认为EWSR1-ETS基因家族易位(范围为61%-96%)属于尤因肉瘤,并会将其纳入尤因肉瘤临床试验的主要分组。对于如何对BCOR-CCNB3、CIC-DUX4以及EWSR1与非ETS伙伴融合进行分类和分层,缺乏共识。大多数受访者要么不确定其所在机构的检测方法,要么其所在机构未进行该项检测。在尤因形态不典型的病例中,大多数受访者倾向于进行额外的融合转录本检测。对于尤因肉瘤中罕见分子亚型的分类和分层缺乏共识。目前尚不清楚这些替代易位对过去临床研究的结果有何影响。这表明需要对诊断进行分子确认,并对检测进行集中化或最低限度的标准化,以便未来进行试验入组。