Drinnon Kyle, Simpson Sean S, Puckett Yana, Ronaghan Catherine A, Richmond Robyn E
Surgery, Texas Tech University Health Sciences Center, Lubbock, USA.
General Surgery, Texas Tech University Health Sciences Center, Lubbock, USA.
Cureus. 2020 Dec 18;12(12):e12156. doi: 10.7759/cureus.12156.
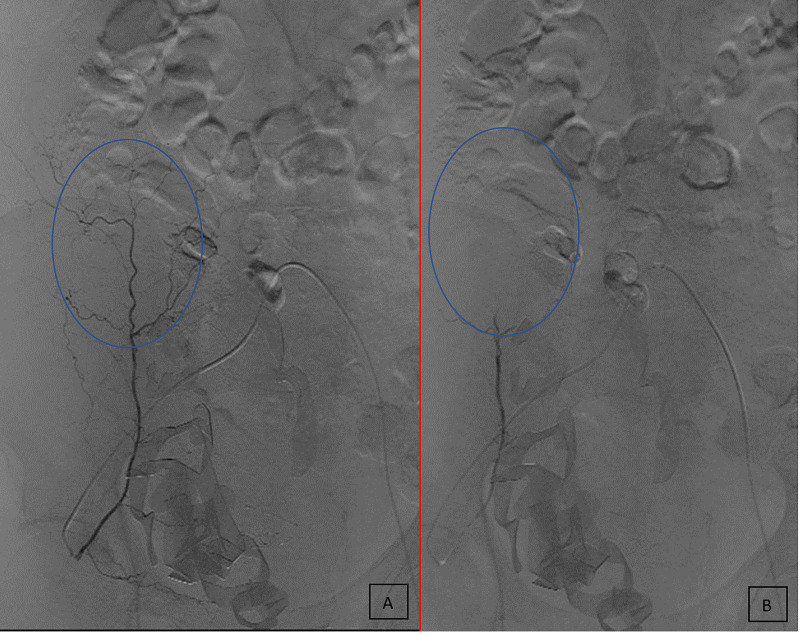
A rectus sheath hematoma (RSH) is a rare medical condition that consists of blood accumulating in the rectus abdominis muscle sheath. RSH is most frequently due to a hemorrhage from the superior or inferior epigastric artery. RSH has many specific risk factors, such as anticoagulant use. As the use of anticoagulants increases, the incidence of RSH has also increased. This condition can present with the infrequent complication of abdominal compartment syndrome (ACS), which can require surgical decompression of the abdomen to avoid high morbidity and mortality. We present the case of a 79-year-old male who, after receiving anticoagulants, developed a right-sided RSH which progressed to ACS. The patient was transferred to our care for community-acquired pneumonia, pneumothorax, and increasing respiratory support. He was admitted to the medical intensive care unit (MICU), was placed on a nasal cannula, and given vancomycin and Zosyn for pneumonia. After two days, the patient was switched to enoxaparin for anticoagulation. After three days, the patient's pneumothorax had resolved. At this time, the patient reported swelling in his right lower quadrant (RLQ) with mild pain, nausea, vomiting, and difficulty voiding completely. The physical examination confirmed RLQ swelling, and a kidney, ureter, and bladder (KUB) x-ray and ultrasound were ordered. A CT with and without contrast was also obtained which showed a large right rectus sheath hematoma extension into preperitoneal space and a small amount of intraperitoneal fluid along the right paracolic gutter. Soon after, the patient became lightheaded and fell after using the restroom. Vitals at the time were a blood pressure of 79/56, heart rate (HR) of 127, and oxygen saturation of 88% with his hemoglobin dropping from 11.4 g/dL earlier that morning to 8.4 g/dL. The patient's care was transferred to our surgical team in the surgical intensive care unit (SICU). He received an arterial line, two doses of protamine, 1-liter of crystalloids, and two units of packed red blood cells (PRBC). The patient's vitals normalized. Interventional radiology (IR) was consulted but they requested the coagulopathy be corrected before any intervention. Reversal of his Lovenox® was thromboelastographic (TEG)-guided and included platelets, cryoprecipitate, and prothrombin complex concentrate/fresh frozen plasma (PCC/FFP), in addition to more PRBCs. During these interventions, the patient acutely decompensated with hypotension, difficulty breathing, and expansion of his hematoma. A bladder pressure in the 30s was obtained, causing him to be sent to the operating room (OR) for decompression, extraperitoneal packing, and the wound was temporarily closed. The patient returned and IR was able to embolize the right inferior epigastric artery. The patient was taken to the OR again for exploration, removal of packing, and closure. RSH is a rare complication that can occur due to trauma, coagulopathy, obesity, and muscle strains during a pregnancy. Larger hematomas tend to occur below the arcuate line because there is an absence of the posterior rectus sheath which enables the hematomas to spread. An RSH can be treated with conservative measures, but for patients who continue to bleed, more aggressive measures should be taken to avoid life-threatening complications, such as ACS.

腹直肌鞘血肿(RSH)是一种罕见的病症,由血液在腹直肌鞘内积聚而成。RSH最常见的原因是来自腹壁上动脉或腹壁下动脉的出血。RSH有许多特定的危险因素,如使用抗凝剂。随着抗凝剂使用的增加,RSH的发病率也有所上升。这种病症可能会出现罕见的并发症——腹腔间隔室综合征(ACS),这可能需要进行腹部手术减压以避免高发病率和死亡率。我们报告一例79岁男性病例,该患者在接受抗凝剂治疗后发生右侧RSH,并进展为ACS。患者因社区获得性肺炎、气胸以及对呼吸支持需求增加而转入我院治疗。他被收入医学重症监护病房(MICU),通过鼻导管吸氧,并给予万古霉素和哌拉西林他唑巴坦治疗肺炎。两天后,患者改用依诺肝素进行抗凝治疗。三天后,患者的气胸已消退。此时,患者报告右下腹(RLQ)肿胀,伴有轻度疼痛、恶心、呕吐以及完全排尿困难。体格检查证实RLQ肿胀,遂安排肾脏、输尿管和膀胱(KUB)X线检查及超声检查。还进行了增强和非增强CT检查,结果显示右侧腹直肌鞘血肿广泛延伸至腹膜前间隙,右侧结肠旁沟有少量腹腔内积液。不久后,患者在使用卫生间后出现头晕并摔倒。当时的生命体征为血压79/56,心率(HR)127,血氧饱和度88%,血红蛋白从当天上午早些时候的11.4 g/dL降至8.4 g/dL。患者的护理工作转至我院外科重症监护病房(SICU)的外科团队。他接受了动脉置管、两剂鱼精蛋白、1升晶体液以及两单位浓缩红细胞(PRBC)。患者的生命体征恢复正常。咨询了介入放射科(IR),但他们要求在进行任何干预之前先纠正凝血功能障碍。停用他的洛伐诺克斯®是在血栓弹力图(TEG)引导下进行的,除了更多的PRBC外,还包括血小板、冷沉淀以及凝血酶原复合物浓缩物/新鲜冰冻血浆(PCC/FFP)。在这些干预过程中,患者突然出现失代偿,伴有低血压、呼吸困难以及血肿扩大。测得膀胱压力为30多,导致他被送往手术室(OR)进行减压、腹膜外填塞,伤口暂时缝合。患者返回后,IR能够栓塞右侧腹壁下动脉。患者再次被送往OR进行探查、取出填塞物并缝合。RSH是一种罕见的并发症,可因创伤、凝血功能障碍、肥胖以及孕期肌肉拉伤而发生。较大的血肿往往发生在弓状线以下,因为此处没有腹直肌后鞘,这使得血肿能够扩散。RSH可以采用保守措施治疗,但对于持续出血的患者,应采取更积极的措施以避免危及生命的并发症,如ACS。