Hematology Department, ICO-IJC-Hospital Germans Trias i Pujol, Badalona, Spain.
Hematology Department, Hospital de Cabueñes, Gijón, Spain.
Cancer Med. 2021 Feb;10(4):1314-1326. doi: 10.1002/cam4.3730. Epub 2021 Jan 25.
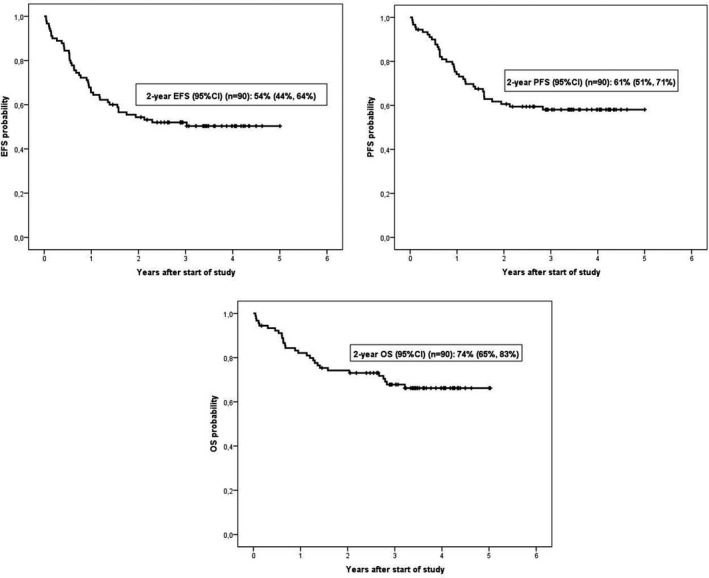
The use of non-pegylated liposomal doxorubicin (Myocet ) in diffuse large B-cell lymphoma (DLBCL) has been investigated in retrospective and single-arm prospective studies. This was a prospective phase 2 trial of DLBCL patients ≥60 years old with left ventricular ejection fraction (LVEF) ≥55% randomized to standard R-CHOP or investigational R-COMP (with Myocet instead of conventional doxorubicin). The primary end point was to evaluate the differences in subclinical cardiotoxicity, defined as decrease in LVEF to <55% at the end of treatment. Secondary objectives were efficacy, safety, and variations of troponin and N-terminal pro-B-type natriuretic peptide (NT-proBNP) and LVEF along follow-up. Ninety patients were included, 45 in each group. No differences were observed in the percentage of patients with LVEF <55% at end of treatment (11% in R-CHOP arm vs. 7% in R-COMP arm, p = 0.697) or at 4 months (10% vs. 6%, respectively, p = 0.667) and 12 months (8% vs. 7%, respectively, p = 1). However, a higher percentage of R-CHOP compared with R-COMP patients showed increased troponin levels in cycle 6 (100% vs. 63%, p = 0.001) and at 1 month after treatment (88% vs. 56%, respectively, p = 0.015). Cardiovascular adverse events were seen in five R-CHOP patients (nine episodes, four grade ≥3) and in four R-COMP patients (five episodes, all grade 1-2). No significant differences in efficacy were observed. In conclusion, R-COMP is a feasible immunochemotherapy schedule for DLBCL patients ≥60 years, with similar efficacy to R-CHOP. However, the use of non-pegylated doxorubicin instead of conventional doxorubicin was not associated with less early cardiotoxicity, although some reduced cardiac safety signals were observed. Trial registration: ClinicalTrials.gov Identifier: NCT02012088.
非聚乙二醇化脂质体多柔比星(Myocet)在弥漫性大 B 细胞淋巴瘤(DLBCL)中的应用已在回顾性和单臂前瞻性研究中进行了研究。这是一项针对年龄≥60 岁、左心室射血分数(LVEF)≥55%的 DLBCL 患者的前瞻性 2 期试验,这些患者被随机分配至标准 R-CHOP 或研究性 R-COMP(用 Myocet 替代常规多柔比星)。主要终点是评估治疗结束时 LVEF 降至<55%的亚临床心脏毒性差异。次要目标是评估疗效、安全性以及随访期间肌钙蛋白和 N 末端 pro-B 型利钠肽(NT-proBNP)和 LVEF 的变化。90 例患者入选,每组 45 例。治疗结束时(R-CHOP 组为 11%,R-COMP 组为 7%,p=0.697)或 4 个月时(分别为 10%和 6%,p=0.667)和 12 个月时(分别为 8%和 7%,p=1),两组中 LVEF<55%的患者比例无差异。然而,与 R-COMP 患者相比,R-CHOP 患者在第 6 周期(100%比 63%,p=0.001)和治疗后 1 个月(88%比 56%,p=0.015)时显示出更高的肌钙蛋白水平升高。在 5 例 R-CHOP 患者(9 例,4 级≥3 级)和 4 例 R-COMP 患者(5 例,均为 1-2 级)中观察到心血管不良事件。两组的疗效无显著差异。总之,R-COMP 是一种适用于年龄≥60 岁的 DLBCL 患者的可行免疫化疗方案,其疗效与 R-CHOP 相当。然而,与常规多柔比星相比,使用非聚乙二醇化多柔比星并未导致早期心脏毒性降低,尽管观察到一些心脏安全性降低的信号。临床试验注册:ClinicalTrials.gov 标识符:NCT02012088。