Elsayed Mei, Christopoulos Petros
Department of Thoracic Oncology, Thoraxklinik and National Center for Tumor Diseases (NCT) at Heidelberg University Hospital, 69126 Heidelberg, Germany.
Translational Lung Research Center Heidelberg (TLRC-H), Member of the German Center for Lung Research (DZL), 69126 Heidelberg, Germany.
Pharmaceuticals (Basel). 2021 Jan 21;14(2):80. doi: 10.3390/ph14020080.
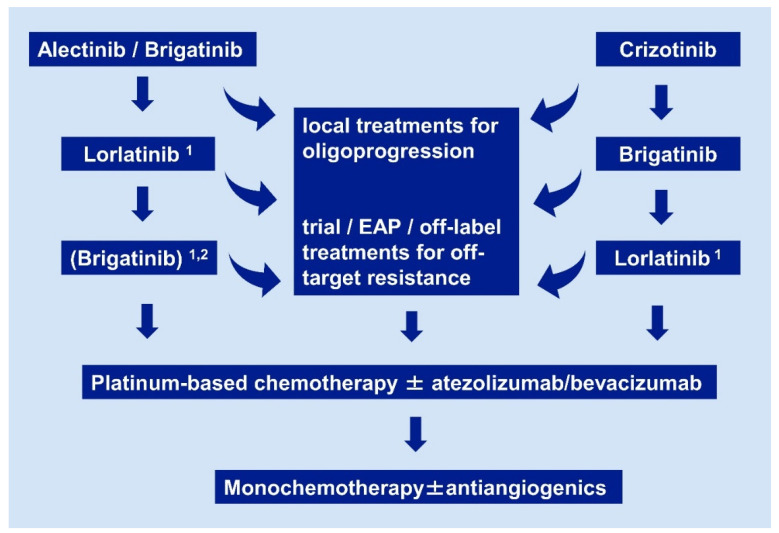
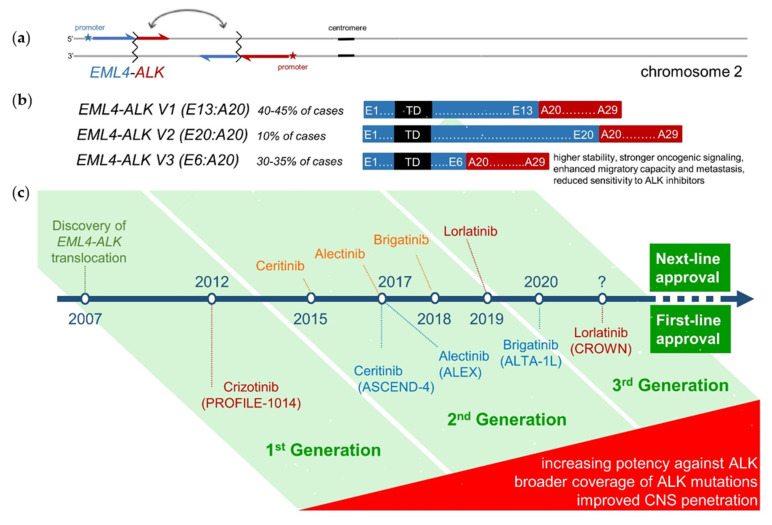
Anaplastic lymphoma kinase-rearranged non-small-cell lung cancer (ALK NSCLC) is a model disease for the use of targeted pharmaceuticals in thoracic oncology. Due to higher systemic and intracranial efficacy, the second-generation ALK tyrosine kinase inhibitors (TKI) alectinib and brigatinib have irrevocably displaced crizotinib as standard first-line treatment, based on the results of the ALEX and ALTA-1L trials. Besides, lorlatinib and brigatinib are the preferred second-line therapies for progression under second-generation TKI and crizotinib, respectively, based on the results of several phase II studies. Tissue or liquid rebiopsies at the time of disease progression, even though not mandated by the approval status of any ALK inhibitor, are gaining importance for individualization and optimization of patient management. Of particular interest are cases with off-target resistance, for example , or alterations, which require special therapeutic maneuvers, e.g., inclusion in early clinical trials or off-label administration of respectively targeted drugs. On the other hand, up to approximately half of the patients failing TKI, develop anatomically restricted progression, which can be initially tackled with local ablative measures without switch of systemic therapy. Among the overall biologically favorable ALK tumors, with a mean tumor mutational burden uniquely below 3 mutations per Mb and the longest survival among NSCLC currently, presence of the fusion variant 3 and/or mutations identify high-risk cases with earlier treatment failure and a need for more aggressive surveillance and treatment strategies. The potential clinical utility of longitudinal ctDNA assays for earlier detection of disease progression and improved guidance of therapy in these patients is a currently a matter of intense investigation. Major pharmaceutical challenges for the field are the development of more potent, fourth-generation TKI and effective immuno-oncological interventions, especially ALK-directed cell therapies, which will be essential for further improving survival and achieving cure of ALK tumors.
间变性淋巴瘤激酶重排的非小细胞肺癌(ALK NSCLC)是胸部肿瘤学中使用靶向药物的典型疾病。基于ALEX和ALTA - 1L试验的结果,由于具有更高的全身和颅内疗效,第二代ALK酪氨酸激酶抑制剂(TKI)阿来替尼和布加替尼已不可逆转地取代克唑替尼成为标准一线治疗药物。此外,根据多项II期研究的结果,洛拉替尼和布加替尼分别是第二代TKI和克唑替尼治疗进展后的首选二线治疗药物。疾病进展时进行组织或液体重新活检,尽管任何ALK抑制剂的获批状态并未强制要求,但对于患者管理的个体化和优化正变得越来越重要。特别值得关注的是具有脱靶耐药性的病例,例如 或 改变,这需要特殊的治疗策略,例如纳入早期临床试验或分别使用靶向药物的超说明书给药。另一方面,高达约一半的TKI治疗失败患者会出现解剖学上局限的进展,最初可以采用局部消融措施处理,而无需更换全身治疗。在总体生物学特性良好的ALK肿瘤中,平均肿瘤突变负荷独特地低于每兆碱基3个突变,并且是目前非小细胞肺癌中生存期最长的,融合变体3和/或 突变的存在可识别出具有早期治疗失败风险且需要更积极监测和治疗策略的高危病例。纵向循环肿瘤DNA(ctDNA)检测在这些患者中用于早期疾病进展检测和改善治疗指导的潜在临床效用目前是深入研究的课题。该领域的主要药物挑战是开发更有效的第四代TKI和有效的免疫肿瘤学干预措施,特别是ALK导向的细胞疗法,这对于进一步提高ALK肿瘤的生存率和实现治愈至关重要。