Intermediate Care Unit, Azienda Ospedaliero-Universitaria Careggi, Florence, Italy.
Internal Medicine, Hospital "Santa Maria Nuova" Florence, Florence, Italy.
BMC Infect Dis. 2021 Jan 25;21(1):116. doi: 10.1186/s12879-021-05781-w.
The burden of cardiovascular (CV) complications in patients hospitalised for community-acquired pneumonia (CAP) is still uncertain. Available studies used different designs and different criteria to define CV complications. We assessed the cumulative incidence of acute of CV complications during hospitalisation for CAP in Internal Medicine Units (IMUs).
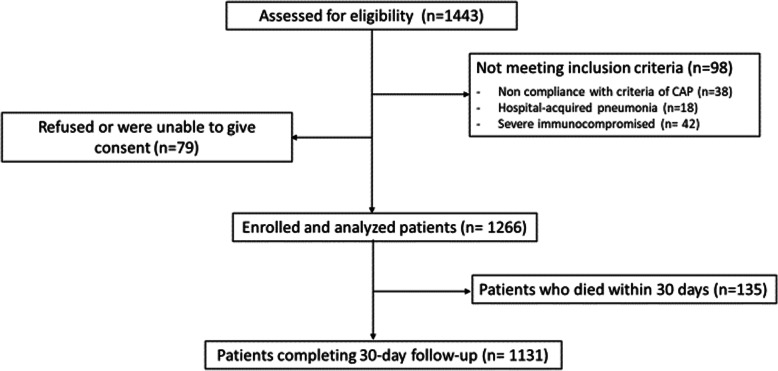
This was a prospective study carried out in 26 IMUs, enrolling patients consecutively hospitalised for CAP. Defined CV complications were: newly diagnosed heart failure, acute coronary syndrome, new onset of supraventricular or ventricular arrhythmias, new onset hemorrhagic or ischemic stroke or transient ischemic attack. Outcome measures were: in-hospital and 30-day mortality, length of hospital stay and rate of 30-day re-hospitalisation.
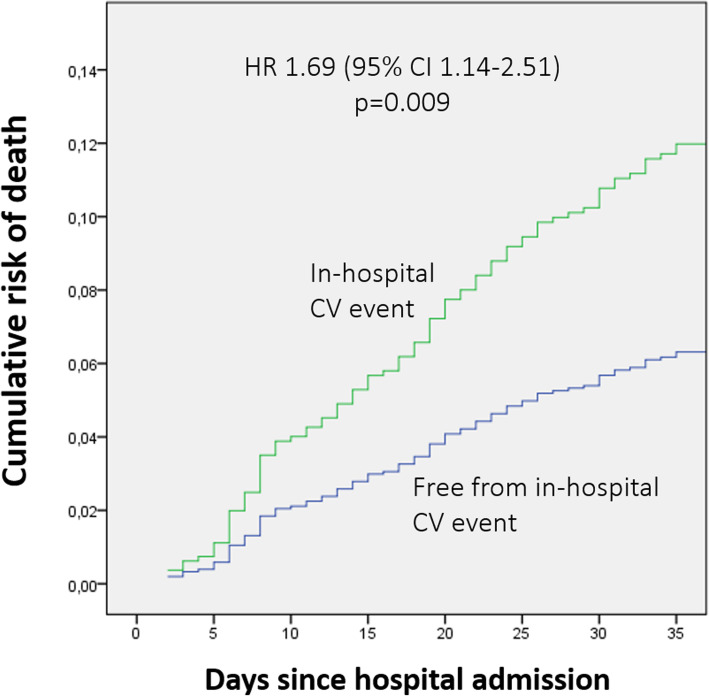
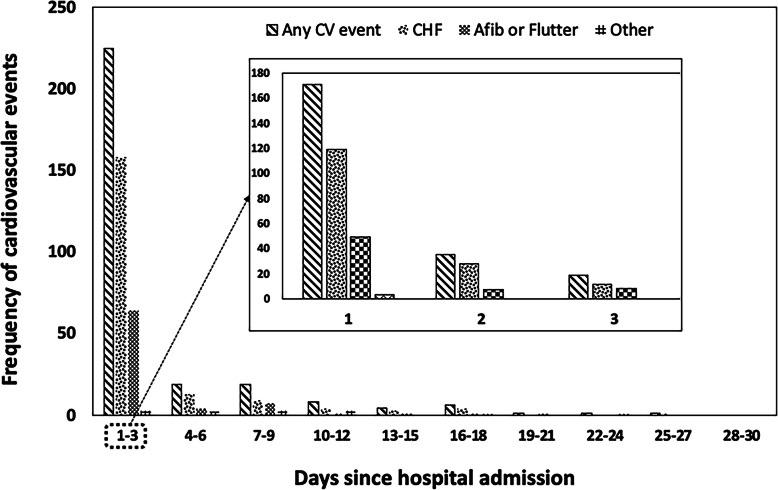
A total of 1266 patients were enrolled, of these 23.8% experienced at least a CV event, the majority (15.5%) represented by newly diagnosed decompensated heart failure, and 75% occurring within 3 days. Female gender, a history of CV disease, and more severe pneumonia were predictors of CV events. In-hospital (12.2% vs 4.7%, p < 0.0001) and 30-day (16.3% vs 8.9%, p = 0.0001) mortality was higher in patients with CV events, as well as the re-hospitalisation rate (13.3% vs 9.3%, p = 0.002), and mean hospital stay was 11.4 ± 6.9 vs 9.5 ± 5.6 days (p < 0.0001). The occurrence of CV events during hospitalisation significantly increased the risk of 30-day mortality (HR 1.69, 95% CI 1.14-2.51; p = 0.009).
Cardiovascular events are frequent in CAP, and their occurrence adversely affects outcome. A strict monitoring might be useful to intercept in-hospital CV complications for those patients with higher risk profile.
NCT03798457 Registered 10 January 2019 - Retrospectively registered.
心血管(CV)并发症在因社区获得性肺炎(CAP)住院的患者中的负担仍不确定。现有研究使用不同的设计和不同的标准来定义 CV 并发症。我们评估了内科病房(IMU)中 CAP 住院期间急性 CV 并发症的累积发生率。
这是一项在 26 个内科病房进行的前瞻性研究,连续纳入因 CAP 住院的患者。定义的 CV 并发症为:新发心力衰竭、急性冠状动脉综合征、新发室上性或室性心律失常、新发出血性或缺血性卒中和短暂性脑缺血发作。主要结局为:住院期间和 30 天死亡率、住院时间和 30 天再住院率。
共纳入 1266 例患者,其中 23.8%至少发生了一次 CV 事件,大多数(15.5%)为新发失代偿性心力衰竭,75%发生在 3 天内。女性、CV 病史和更严重的肺炎是 CV 事件的预测因素。CV 事件患者的住院(12.2%比 4.7%,p<0.0001)和 30 天死亡率(16.3%比 8.9%,p=0.0001)以及再住院率(13.3%比 9.3%,p=0.002)更高,平均住院时间为 11.4±6.9 天比 9.5±5.6 天(p<0.0001)。住院期间发生 CV 事件显著增加了 30 天死亡率的风险(HR 1.69,95%CI 1.14-2.51;p=0.009)。
CV 事件在 CAP 中很常见,其发生会对预后产生不利影响。对于那些具有更高风险特征的患者,严格监测可能有助于拦截住院期间的 CV 并发症。
NCT03798457 于 2019 年 1 月 10 日注册-回顾性注册。