Department of Anesthesiology and Intensive Care, Falun Hospital, Falun, Sweden.
Center for Clinical Research Dalarna-Uppsala University, Falun, Sweden.
J Ultrasound Med. 2021 Nov;40(11):2339-2351. doi: 10.1002/jum.15617. Epub 2021 Jan 26.
Indication for invasive mechanical ventilation in COVID-19 pneumonia has been a major challenge. This study aimed to evaluate if lung ultrasound (LUS) can assist identification of requirement of invasive mechanical ventilation in moderate to severe COVID-19 pneumonia.
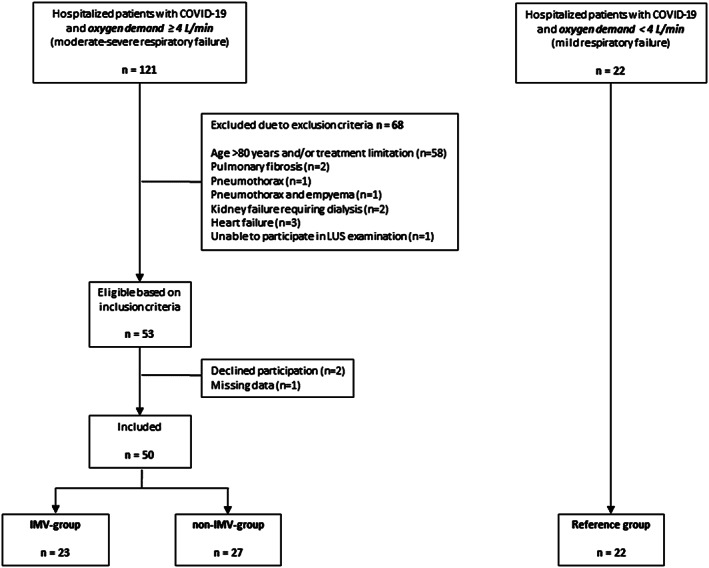
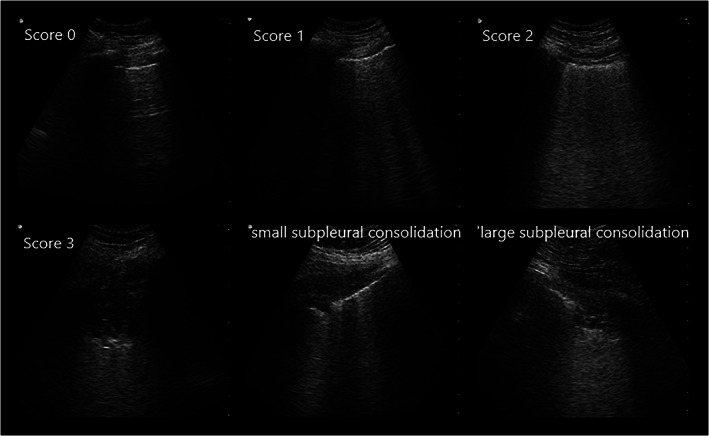
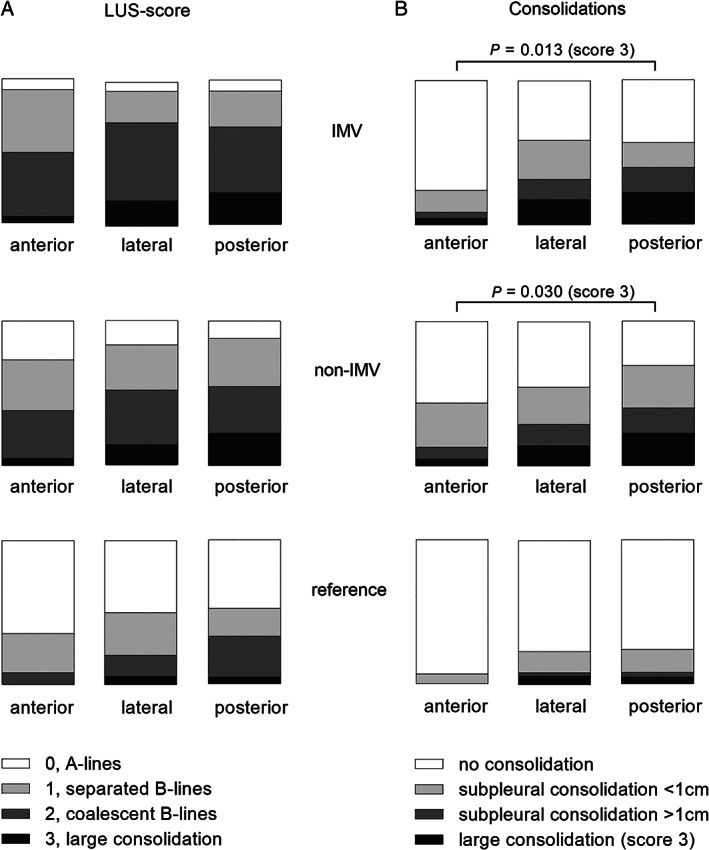
Between April 23 and November 12, 2020, hospitalized patients with moderate to severe COVID-19 (oxygen demand ≥4 L/min) were included consecutively. Lung ultrasound was performed daily until invasive mechanical ventilation (IMV-group) or spontaneous recovery (non-IMV-group). Clinical parameters and lung ultrasound findings were compared between groups, at intubation (IMV-group) and highest oxygen demand (non-IMV-group). A reference group with oxygen demand <4 L/min was examined at hospital admission.
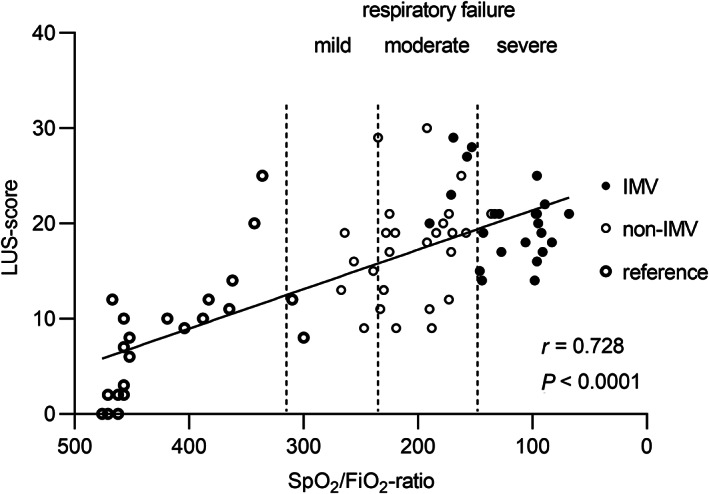
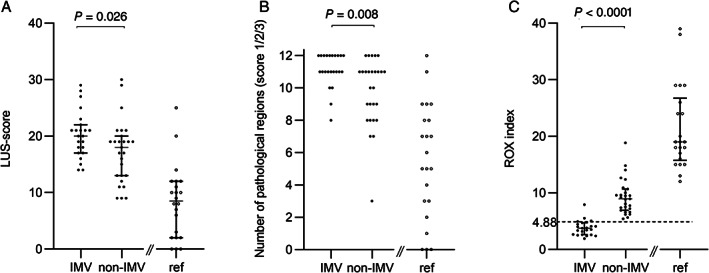
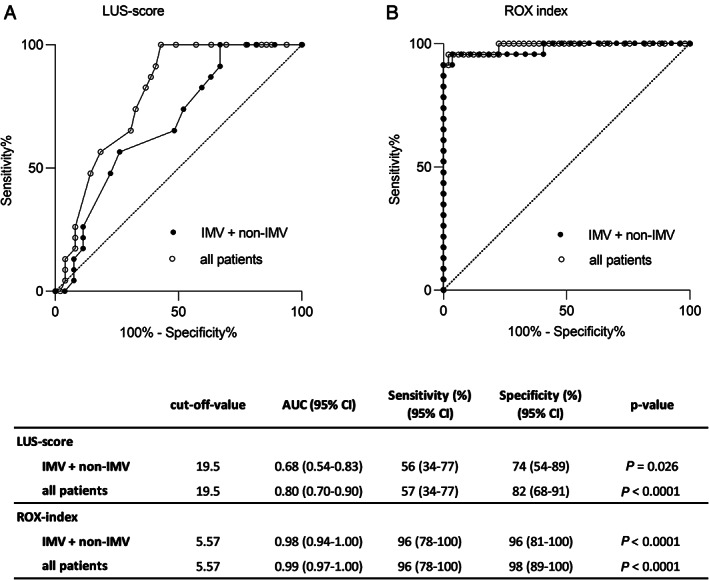
Altogether 72 patients were included: 50 study patients (IMV-group, n = 23; non-IMV-group, n = 27) and 22 reference patients. LUS-score correlated to oxygen demand (SpO /FiO -ratio) (r = 0.728; p < .0001) and was higher in the IMV-group compared to the non-IMV-group (20.0 versus 18.0; p = .026). Based on receiver operating characteristic analysis, a LUS-score of 19.5 was identified as cut-off for requirement of invasive mechanical ventilation (area under the curve 0.68; sensitivity 56%, specificity 74%). In 6 patients, LUS identified critical coexisting conditions. Respiratory rate and oxygenation index ((SpO /FiO )/respiratory rate) ≥4.88 identified no requirement of invasive mechanical ventilation with a positive predictive value of 87% and negative predictive value of 100%.
LUS-score had only a moderate diagnostic value for requirement of invasive mechanical ventilation in moderate to severe COVID-19. However, LUS proved valuable as complement to respiratory parameters in guidance of disease severity and identifying critical coexisting conditions.
COVID-19 肺炎患者有创机械通气的适应证一直是一个主要的挑战。本研究旨在评估肺部超声(LUS)是否可以辅助识别中重度 COVID-19 肺炎患者有创机械通气的需求。
2020 年 4 月 23 日至 11 月 12 日,连续纳入中重度 COVID-19(需氧≥4L/min)住院患者。在有创机械通气(IMV 组)或自发恢复(非 IMV 组)前,每天进行肺部超声检查。比较两组患者的临床参数和肺部超声表现,在插管时(IMV 组)和最高需氧量时(非 IMV 组)进行比较。同时检查氧气需求<4L/min 的参考组。
共纳入 72 例患者:50 例研究患者(IMV 组,n=23;非 IMV 组,n=27)和 22 例参考患者。LUS 评分与氧合指数(SpO /FiO 比值)相关(r=0.728;p<0.0001),且在 IMV 组中高于非 IMV 组(20.0 与 18.0;p=0.026)。基于受试者工作特征分析,19.5 的 LUS 评分被确定为需要有创机械通气的截断值(曲线下面积 0.68;敏感性 56%,特异性 74%)。在 6 例患者中,LUS 识别出了关键共存疾病。呼吸频率和氧合指数[(SpO /FiO )/呼吸频率]≥4.88 可预测无有创机械通气需求,阳性预测值为 87%,阴性预测值为 100%。
LUS 评分对中重度 COVID-19 患者有创机械通气的需求只有中等的诊断价值。然而,LUS 作为呼吸参数的补充,在指导疾病严重程度和识别关键共存疾病方面具有重要价值。