Department of Pediatric Hematology and Oncology, Oslo University Hospital, Oslo, Norway.
Division of Oncology, Center for Childhood Cancer Research and Cancer Immunotherapy Program, Children's Hospital of Philadelphia, Philadelphia, PA.
Blood Adv. 2021 Jan 26;5(2):593-601. doi: 10.1182/bloodadvances.2020002757.
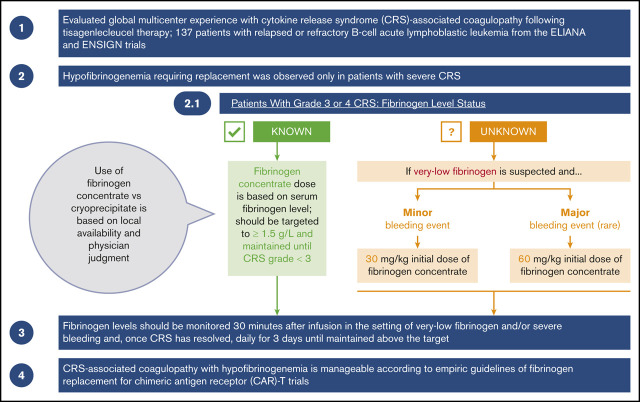
Cytokine release syndrome (CRS) is a systemic inflammatory response associated with chimeric antigen receptor T-cell (CAR-T) therapies. In severe cases, CRS can be associated with coagulopathy and hypofibrinogenemia. We present our global multicenter experience with CRS-associated coagulopathy after tisagenlecleucel therapy in 137 patients with relapsed or refractory B-cell acute lymphoblastic leukemia from the ELIANA and ENSIGN trials. These trials included clinical guidelines for fibrinogen replacement during CRS-associated coagulopathy. Hypofibrinogenemia requiring replacement was observed only in patients with severe CRS. A higher percentage of patients who required replacement were <10 years old, compared with those who did not require replacement. Twenty-three patients received replacement for hypofibrinogenemia (<1.5 g/L); 9 of them developed marked hypofibrinogenemia (<1 g/L). Very low fibrinogen levels (<1 g/L) were documented in patients before maximal CRS (n = 1), during maximal CRS (n = 7), and at CRS improvement (n = 1). Although hypofibrinogenemia was the most clinically significant coagulopathy, some patients also developed prolonged prothrombin time and activated partial thromboplastin time and increased international normalized ratio, further increasing the risk of bleeding. Hypofibrinogenemia was effectively managed using fibrinogen concentrate or cryoprecipitate replacement; severe (grade 4) bleeding events were rare (n = 2). CRS-associated coagulopathy with hypofibrinogenemia is manageable according to empiric guidelines of fibrinogen replacement for CAR-T trials. Fibrinogen concentrate should be used when cryoprecipitate is not reliably available. Monitoring fibrinogen levels in patients with moderate or severe CRS is essential for avoiding potentially fatal bleeding events. These trials were registered at www.clinicaltrials.gov as #NCT02435849 and #NCT02228096.
细胞因子释放综合征(CRS)是一种与嵌合抗原受体 T 细胞(CAR-T)疗法相关的全身性炎症反应。在严重的情况下,CRS 可能与凝血障碍和低纤维蛋白原血症有关。我们报告了在 ELIANA 和 ENSIGN 试验中,137 例复发或难治性 B 细胞急性淋巴细胞白血病患者接受 tisagenlecleucel 治疗后,与 CRS 相关的凝血障碍的全球多中心经验。这些试验包括 CRS 相关凝血障碍时纤维蛋白原替代的临床指南。仅在发生严重 CRS 的患者中观察到需要替代的低纤维蛋白原血症。需要替代的患者中,年龄小于 10 岁的比例高于不需要替代的患者。23 例患者因低纤维蛋白原血症(<1.5 g/L)接受替代治疗;其中 9 例出现明显低纤维蛋白原血症(<1 g/L)。在 CRS 最大程度改善时(n=1)、在 CRS 改善时(n=1)和在 CRS 最大程度时(n=7),患者的纤维蛋白原水平非常低(<1 g/L)。尽管低纤维蛋白原血症是最具临床意义的凝血障碍,但一些患者还出现了延长的凝血酶原时间和活化部分凝血活酶时间以及国际标准化比值增加,进一步增加了出血风险。低纤维蛋白原血症通过纤维蛋白原浓缩物或冷沉淀替代物有效治疗;严重(4 级)出血事件很少见(n=2)。根据 CAR-T 试验纤维蛋白原替代的经验指南,可管理与 CRS 相关的低纤维蛋白原血症伴凝血障碍。在冷沉淀不可靠时,应使用纤维蛋白原浓缩物。监测中重度 CRS 患者的纤维蛋白原水平对于避免潜在致命的出血事件至关重要。这些试验在 www.clinicaltrials.gov 上注册为 #NCT02435849 和 #NCT02228096。