Division of Hepatology, Department of Internal Medicine, Iwate Medical University School of Medicine, Shiwa, Iwate, Japan.
Department of Gastroenterology, Morioka City Hospital, Morioka, Iwate, Japan.
Am J Case Rep. 2021 Jan 28;22:e928587. doi: 10.12659/AJCR.928587.
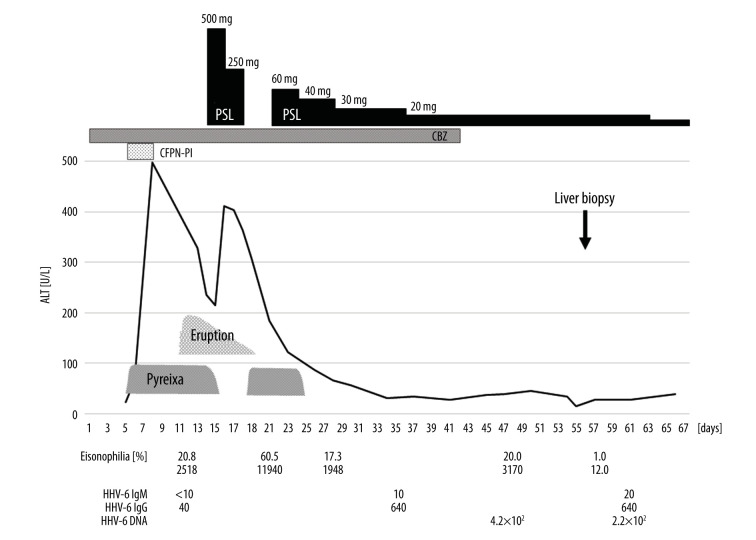
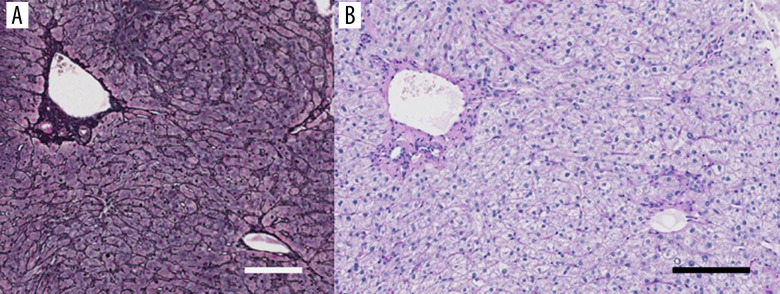
BACKGROUND Infection with human herpesvirus 6 (HHV-6) is a recognized risk factor for the development of drug-induced hypersensitivity syndrome (DIHS). DIHS is a systemic autoimmune condition that presents with mucocutaneous lesions of varying severity and comprises 3 subtypes: toxic epidermal necrolysis, Stevens-Johnson syndrome, and drug reaction with eosinophilia and systemic symptoms (DRESS). Here, we describe the case of a 51-year-old woman with a diagnosis of DIHS associated with carbamazepine, reactivation of HHV-6, and acute liver failure, which was consistent with DRESS. CASE REPORT We present the case of a 51-year-old Japanese woman who had been taking carbamazepine for epilepsy for the past 3 weeks. She presented with a fever, liver dysfunction, eosinophilia, and the sudden appearance of a skin rash. Steroid therapy was started for suspected drug-induced liver injury. The skin eruption disappeared, and liver dysfunction showed an improving trend. However, after stopping steroid, the pyrexia and eosinophilia reappeared. Therefore, prednisolone was re-administrated. HHV-6 DNA was detected, so HHV-6 reactivation was confirmed. Carbamazepine was stopped, and the clinical manifestations improved. She was ultimately diagnosed with DIHS, consistent with DRESS, associated with carbamazepine and HHV-6 reactivation, and liver dysfunction was assessed histologically. Therefore, the drug-related hepatotoxicity of carbamazepine played a role in causing liver damage rather than HHV-6 infection at that time. CONCLUSIONS We describe a case of DIHS that was also associated with acute liver failure, consistent with DRESS. The case highlights the importance of making the correct diagnosis, as well as the management of mucocutaneous lesions and other systemic conditions (including acute liver failure).
人类疱疹病毒 6 型(HHV-6)感染是药物诱导超敏综合征(DIHS)发展的公认危险因素。DIHS 是一种系统性自身免疫性疾病,表现为不同严重程度的黏膜皮肤损伤,包括 3 个亚型:中毒性表皮坏死松解症、史蒂文斯-约翰逊综合征和药物反应伴嗜酸性粒细胞增多和全身症状(DRESS)。在此,我们描述了一例 51 岁女性患者,诊断为与卡马西平相关的 DIHS,HHV-6 再激活和急性肝衰竭,符合 DRESS。
我们介绍了一例 51 岁日本女性患者,她因癫痫一直在服用卡马西平,过去 3 周内出现发热、肝功能异常、嗜酸性粒细胞增多和皮疹突然出现。因疑似药物性肝损伤开始给予类固醇治疗。皮疹消退,肝功能呈改善趋势。然而,停用类固醇后,发热和嗜酸性粒细胞增多再次出现。因此,重新给予泼尼松龙。检测到 HHV-6 DNA,因此确认 HHV-6 再激活。停用卡马西平后,临床症状改善。最终诊断为 DIHS,符合 DRESS,与卡马西平及 HHV-6 再激活相关,且肝组织学检查显示肝功能异常。因此,卡马西平的药物相关性肝毒性在当时起了导致肝损伤的作用,而非 HHV-6 感染。
我们描述了一例 DIHS 病例,也伴有急性肝衰竭,符合 DRESS。该病例强调了正确诊断的重要性,以及黏膜皮肤病变和其他全身情况(包括急性肝衰竭)的管理。