Rodriguez Jose A, Bonnano Charles, Khatiwada Pratik, Roa Alejandra A, Mayer Daniel, Eckardt Paula A
Department of Internal Medicine, Memorial Healthcare System, Pembroke Pines, FL, USA.
Division of Critical Care Memorial Hospital West, Memorial Healthcare, Pembroke Pines, FL, USA.
Case Rep Infect Dis. 2021 Jan 15;2021:8840536. doi: 10.1155/2021/8840536. eCollection 2021.
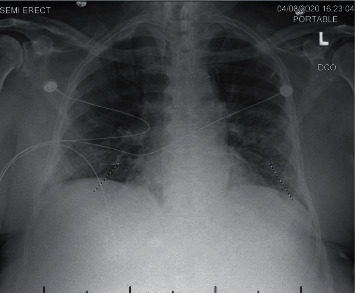
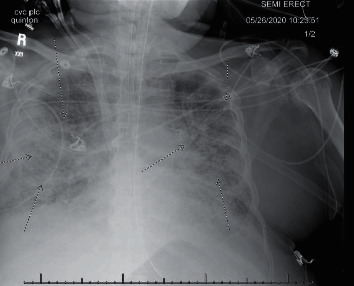
Coronavirus disease (COVID-19) is a worldwide pandemic causing multiple fatalities and morbidities worldwide. We report a case of severe pneumonia causing acute respiratory distress syndrome due to a coinfection with SARS-CoV-2 and in an elderly patient with multiple myeloma in Florida, USA. . An 84-year-old male with a medical history significant for multiple myeloma not in remission was sent to the emergency department to rule out COVID-19 infection prior to continuing his chemotherapy sessions. At presentation, he had nonspecific mild symptoms and an unremarkable physical examination. He had significant blood test findings including serum lactate dehydrogenase 373 U/L, high sensitive C-reactive protein 17.40 mg/l, and ferritin 415 ng/ml. Xpert-SARS-CoV-2 was positive. Chest radiograph revealed patchy areas of interstitial infiltrates in mid to lower lung zones. During his hospitalization course, his oxygenation deteriorated, requiring mechanical intubation. Repeat chest radiograph showed worsening bilateral infiltrates. He was started on broad-spectrum antibiotics and eventually weaned off mechanical intubation and extubated. On the 11 day of admission, he was found to be bradycardic and in shock, and he was reintubated. His labs showed worsening inflammatory markers along with kidney dysfunction to the point of requiring renal replacement therapy. He received both convalescent plasma and remdesivir for treatment of COVID-19 pneumonia. Eventually, repeat blood cultures came back positive for the growth of acid-fast beaded bacilli. While awaiting final culture and sensitivity reports, his antibiotics were upgraded to cover possible nocardia infection. Repeat blood and sputum cultures resulted in growth of AFB bacilli 1 week after.
This case report highlights the importance of keeping a broad differential and considering multiple coinfections, including atypical ones during this COVID-19 pandemic, such as the one that was discussed above, , in order to provide goal-directed therapy.
冠状病毒病(COVID-19)是一场全球大流行疾病,在全球范围内导致了多起死亡和发病案例。我们报告了美国佛罗里达州一名患有多发性骨髓瘤的老年患者因感染严重急性呼吸综合征冠状病毒2(SARS-CoV-2)合并感染而导致严重肺炎并引发急性呼吸窘迫综合征的病例。一名84岁男性,有显著的多发性骨髓瘤病史且病情未缓解,在继续化疗前被送往急诊科以排除COVID-19感染。就诊时,他有非特异性轻度症状,体格检查无异常。他的血液检查结果显著,包括血清乳酸脱氢酶373 U/L、高敏C反应蛋白17.40 mg/l和铁蛋白415 ng/ml。Xpert-SARS-CoV-2检测呈阳性。胸部X线片显示中至下肺区有斑片状间质浸润。在住院期间,他的氧合情况恶化,需要机械通气。复查胸部X线片显示双侧浸润加重。他开始接受广谱抗生素治疗,最终脱机拔管。入院第11天,他出现心动过缓和休克,再次插管。他的实验室检查显示炎症指标恶化,同时出现肾功能障碍,需要进行肾脏替代治疗。他接受了恢复期血浆和瑞德西韦治疗COVID-19肺炎。最终,重复血培养结果显示抗酸串珠杆菌生长呈阳性。在等待最终培养和药敏报告期间,他的抗生素升级以覆盖可能的诺卡菌感染。1周后,重复血液和痰培养结果显示抗酸杆菌生长。
本病例报告强调了在COVID-19大流行期间保持广泛鉴别诊断并考虑多种合并感染(包括非典型感染,如上述讨论的感染)的重要性,以便提供目标导向治疗。