Huebinger Ryan M, Walia Shabana, Yealy Donald M, Kellum John A, Huang David T, Wang Henry E
Department of Emergency Medicine McGovern Medical School at The University of Texas Health Science Center at Houston (UTHealth) Houston Texas USA.
Department of Emergency Medicine University of Pittsburgh Pittsburgh Pennsylvania USA.
J Am Coll Emerg Physicians Open. 2021 Jan 18;2(1):e12358. doi: 10.1002/emp2.12358. eCollection 2021 Feb.
Intravenous fluid administration is a main component of sepsis therapy, but physicians are cautious about giving fluids to end-stage renal disease (ESRD) patients out of concern for causing volume overload. We compared the outcomes of septic shock patients with and without ESRD and evaluated the association between early intravenous fluid administration and outcomes.
We analyzed patients enrolled in the Protocolized Care for Early Septic Shock (PROCESS) trial, which studied different resuscitation strategies for early septic shock. Stratifying for ESRD, we compared patient characteristics, course of care, and outcomes between ESRD and non-ESRD. Using multivariable logistic regression, we determined the association between 6-hour total fluid volume (> = 30 mL/kg vs < 30 mL/kg) from preenrollment and outcomes.
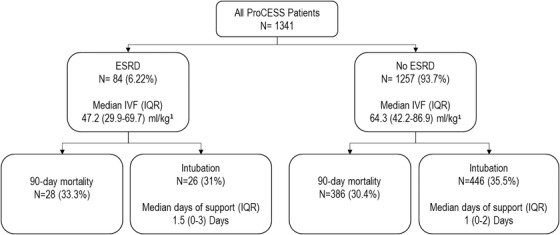
There were 84 ESRD and 1257 non-ESRD patients. ESRD patients had a higher median Charlson Comorbidity score (5 vs 2, < .001), higher median acute physiology and chronic health evaluation (APACHE) II score (26.5 vs 20.0, < .001), and lower 6-hour intravenous fluid administration (54.7 vs 68.3 mL/kg, < .001). Ninety-day mortality (33.3% vs 29.3%, = .43) and intubation rate (31.0% vs 33.4%, = .64) did not differ between groups. Fewer ESRD received > = 30 mL/kg (66.6% vs 86.7% < .001). For ESRD, receipt of > = 30 mL/kg intravenous fluid did not alter any outcome. For non-ESRD patients, receiving ≥30 mL/kg of intravenous fluid was associated with increased 90-day mortality (adjusted odds ratio = 1.64; 95% confidence interval, 1.03-2.61).
In the PROCESS trial, ESRD patients had similar outcomes to non-ESRD patients. Although ESRD patients received less intravenous fluid administration, most received over 30 mL/kg in the first 6 hours. In contrast to non-ESRD patients, receiving ≥30 mL/kg of intravenous fluid was not associated with worse outcomes in ESRD.
静脉输液是脓毒症治疗的主要组成部分,但医生因担心导致容量超负荷而对终末期肾病(ESRD)患者输液持谨慎态度。我们比较了患有和未患有ESRD的感染性休克患者的结局,并评估了早期静脉输液与结局之间的关联。
我们分析了参与早期感染性休克标准化治疗(PROCESS)试验的患者,该试验研究了早期感染性休克的不同复苏策略。按ESRD进行分层,我们比较了ESRD组和非ESRD组患者的特征、治疗过程及结局。使用多变量逻辑回归,我们确定了入组前6小时总输液量(≥30 mL/kg与<30 mL/kg)与结局之间的关联。
共有84例ESRD患者和1257例非ESRD患者。ESRD患者的Charlson合并症评分中位数更高(5比2,P<0.001),急性生理学与慢性健康状况评分(APACHE)II评分中位数更高(26.5比20.0,P<0.001),且6小时静脉输液量更低(54.7比68.3 mL/kg,P<0.001)。两组间90天死亡率(33.3%比29.3%,P = 0.43)和插管率(31.0%比33.4%,P = 0.64)无差异。接受≥30 mL/kg的ESRD患者更少(66.6%比86.7%,P<0.001)。对于ESRD患者,接受≥30 mL/kg静脉输液并未改变任何结局。对于非ESRD患者,接受≥30 mL/kg静脉输液与90天死亡率增加相关(调整后的优势比=1.64;95%置信区间,1.03 - 2.61)。
在PROCESS试验中,ESRD患者与非ESRD患者结局相似。尽管ESRD患者接受的静脉输液量较少,但大多数患者在最初6小时内接受了超过30 mL/kg的输液量。与非ESRD患者不同,ESRD患者接受≥30 mL/kg静脉输液与更差的结局无关。