Department of General Thoracic Surgery, Jichi Medical University, 3311-1 Yakushiji, Shimotsuke, Tochigi, 329-0498, Japan.
Department of General Thoracic Surgery, Jichi Medical University Saitama Medical Center, Saitama, Saitama, Japan.
Gen Thorac Cardiovasc Surg. 2021 Jul;69(7):1096-1104. doi: 10.1007/s11748-021-01585-6. Epub 2021 Jan 28.
Selection criteria for palliative limited surgery in patients with non-small cell lung cancer (NSCLC) can vary by institution or surgeon. We retrospectively reviewed outcomes of poor-risk patients who underwent palliative segmentectomy (PS), using the National Clinical Database Risk Calculator (RC).
We retrospectively analyzed medical records of patients with NSCLC tumors ≥ 20 mm and consolidation/tumor ratios ≥ 0.5 on computed tomography, who underwent PS from January 2009 to March 2016. Median follow-up time was 47 months (range 2-102 months).
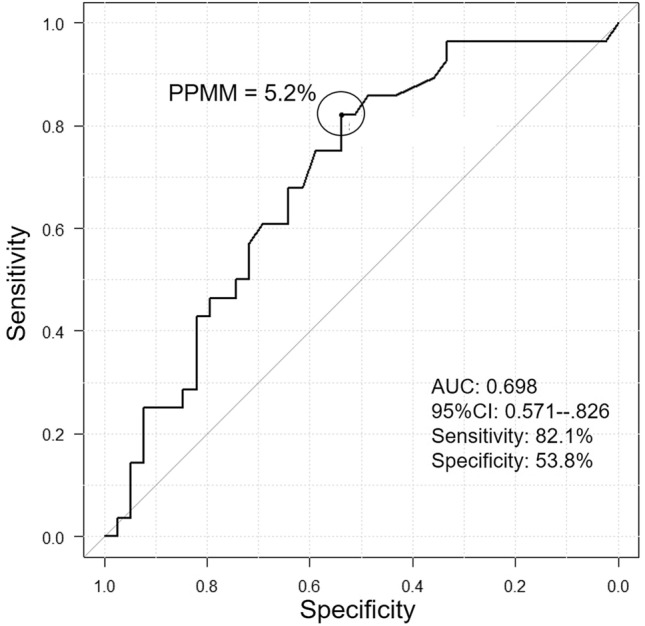
We enrolled 67 patients (median age: 73.0 years), of whom 54 received thoracoscopic surgery and 28 received medial lymph-node dissection. The RC's mean predictive probability rate for perioperative mortality or severe complications was 7.1%. Of the 67 patients, 24 patients (43.0%) suffered post-surgical complications, including 2 (3%) who died in hospital; 17 eventually suffered NSCLC recurrences and/or metastases, 11 eventually died from NSCLC, and 17 died from other diseases. Five-year overall survival (OS) was 59.4%. When the patients were divided into high-risk (HR) and low-risk (LR) groups based on the RC, 5-year OS was significantly less in the HR group (43.9%) than in the LR group (82.2%; P < 0.05).
The RC, which was developed primarily to determine perioperative risk, can predict long-term prognosis for compromised patients who undergo PS.
非小细胞肺癌(NSCLC)患者行姑息性局限性肺切除术(PS)的选择标准可能因机构或外科医生而异。我们使用国家临床数据库风险计算器(RC)回顾性分析了接受姑息性节段切除术(PS)的高危患者的结果。
我们回顾性分析了 2009 年 1 月至 2016 年 3 月期间接受 PS 的 NSCLC 肿瘤≥20mm 和 CT 上实变/肿瘤比≥0.5 的患者的病历。中位随访时间为 47 个月(范围 2-102 个月)。
我们纳入了 67 例患者(中位年龄:73.0 岁),其中 54 例行胸腔镜手术,28 例行中纵隔淋巴结清扫术。RC 预测围手术期死亡率或严重并发症的平均预测概率为 7.1%。67 例患者中有 24 例(43.0%)发生术后并发症,包括 2 例(3%)在院死亡;17 例最终发生 NSCLC 复发和/或转移,11 例最终死于 NSCLC,17 例死于其他疾病。5 年总生存率(OS)为 59.4%。根据 RC 将患者分为高危(HR)和低危(LR)组后,HR 组的 5 年 OS 明显低于 LR 组(43.9%vs82.2%;P<0.05)。
RC 主要用于确定围手术期风险,可预测行 PS 的高危患者的长期预后。