Menzies School of Health Research, Wellbeing and Preventable Chronic Diseases Division, Charles Darwin University, Darwin, Northern Territory, Australia.
School of Psychological and Clinical Sciences, Charles Darwin University, Darwin, Northern Territory, Australia.
BMC Health Serv Res. 2021 Jan 28;21(1):95. doi: 10.1186/s12913-021-06066-3.
Poorer cancer outcomes of Indigenous Australians in Australia's Northern Territory (NT) compared with their non-Indigenous counterparts are partially due to diminished access to cancer treatment services (CTS). Accessibility of health care is a multidimensional construct, including physical, logistical, psychosocial and cultural dimensions. While previous research has identified specific areas of reduced access to CTS for Indigenous Australians, the higher burden of cancer borne by Indigenous Australians warrants a more comprehensive understanding of access to CTS in the NT. The purpose of this study was to explore and map the accessibility of CTS for Indigenous Australians in the NT and to identify key access barriers.
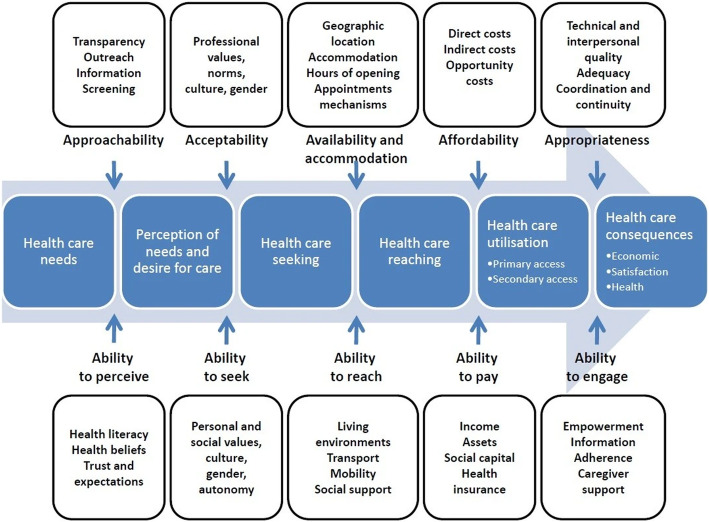
This predominantly qualitative study, complemented by a descriptive quantitative component, explored and mapped the accessibility of one CTS (CTS-NT) that services a large number of Indigenous Australians in the NT. Patient perspectives were obtained via secondary analysis of data from 75 face-to-face interviews with Indigenous Australian adults attending the CTS-NT. Care provider perspectives were obtained via primary analysis of data from 29 face-to-face interviews with care providers and staff working at CTS-NT. Data were analysed to identify issues of accessibility informed by Leveque and colleagues' conceptual framework of access to health care, which comprises five dimensions of accessibility of the health service and the ability of Indigenous patients to interact with these dimensions to generate access. Applied thematic analysis was conducted on the qualitative data and descriptive analysis was conducted on the quantitative data.
The analysis of the patient and care provider reports identified multiple access barriers across all dimensions including: inadequate preparation of Indigenous patients for treatment; delayed and complicated commencement of treatment; dislocation from home; competing priorities; scarcity of Indigenous care providers and staff; lack of culturally-relevant care; challenges associated with language, accommodation, transport and finance; and disjointed and fraught relationships with care providers. These barriers posed significant challenges to Indigenous patients maintaining their engagement with treatment.
This study provides a valuable snapshot of the barriers facing this population across the dimensions of health care access. Urgent action in addressing these issues is required at individual, service and state levels.
与非原住民相比,澳大利亚北部地区(NT)的土著澳大利亚人癌症预后较差,部分原因是他们获得癌症治疗服务(CTS)的机会减少。医疗保健的可及性是一个多维的概念,包括物理、后勤、心理社会和文化方面。虽然之前的研究已经确定了土著澳大利亚人获得 CTS 的机会减少的具体领域,但土著澳大利亚人所承担的更高的癌症负担需要对 NT 地区获得 CTS 的情况有更全面的了解。本研究的目的是探讨和描绘 NT 地区土著澳大利亚人获得 CTS 的便利性,并确定关键的准入障碍。
本研究主要采用定性方法,并辅以描述性定量部分,探讨和描绘了为 NT 地区大量土著澳大利亚人服务的一种 CTS(CTS-NT)的可及性。通过对参加 CTS-NT 的 75 名土著澳大利亚成年人的 75 次面对面访谈的二次分析,获得了患者的观点。通过对在 CTS-NT 工作的护理提供者和工作人员的 29 次面对面访谈的原始分析,获得了护理提供者的观点。根据 Leveque 等人的医疗保健可及性概念框架,分析数据以识别可及性问题,该框架包括卫生服务可及性的五个维度以及土著患者与这些维度互动以产生可及性的能力。对定性数据进行应用主题分析,对定量数据进行描述性分析。
对患者和护理提供者报告的分析确定了所有维度的多个准入障碍,包括:土著患者接受治疗的准备不足;治疗开始延迟且复杂;被迫离开家乡;优先事项相互竞争;土著护理提供者和工作人员稀缺;缺乏文化相关的护理;与语言、住宿、交通和资金相关的挑战;以及与护理提供者的关系脱节和紧张。这些障碍给土著患者坚持治疗带来了巨大挑战。
本研究提供了该人群在医疗保健可及性各个维度面临的障碍的宝贵快照。需要在个人、服务和州各级紧急解决这些问题。