Department of Biological Sciences, University of Notre Dame, Notre Dame, Indiana.
Center for Healthcare Equity in Kidney Disease, University of New Mexico Health Sciences Center, Albuquerque, New Mexico.
Clin J Am Soc Nephrol. 2021 Feb 8;16(2):262-274. doi: 10.2215/CJN.04860420. Epub 2021 Jan 28.
Black patients have a higher incidence of kidney failure but lower rate of deceased- and living-donor kidney transplantation compared with White patients, even after taking differences in comorbidities into account. We assessed whether social determinants of health (., demographics, cultural, psychosocial, knowledge factors) could account for race differences in receiving deceased- and living-donor kidney transplantation.
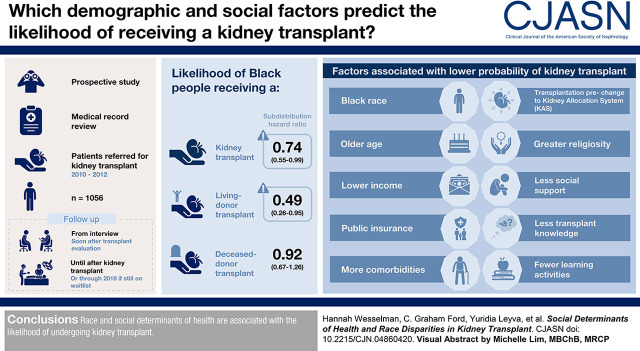
DESIGN, SETTING, PARTICIPANTS, & MEASUREMENTS: medical record review, we prospectively followed 1056 patients referred for kidney transplant (2010-2012), who completed an interview soon after kidney transplant evaluation, until their kidney transplant. We used multivariable competing risk models to estimate the cumulative incidence of receipt of any kidney transplant, deceased-donor transplant, or living-donor transplant, and the factors associated with each outcome.
Even after accounting for social determinants of health, Black patients had a lower likelihood of kidney transplant (subdistribution hazard ratio, 0.74; 95% confidence interval, 0.55 to 0.99) and living-donor transplant (subdistribution hazard ratio, 0.49; 95% confidence interval, 0.26 to 0.95), but not deceased-donor transplant (subdistribution hazard ratio, 0.92; 95% confidence interval, 0.67 to 1.26). Black race, older age, lower income, public insurance, more comorbidities, being transplanted before changes to the Kidney Allocation System, greater religiosity, less social support, less transplant knowledge, and fewer learning activities were each associated with a lower probability of any kidney transplant. Older age, more comorbidities, being transplanted before changes to the Kidney Allocation System, greater religiosity, less social support, and fewer learning activities were each associated with a lower probability of deceased-donor transplant. Black race, older age, lower income, public insurance, higher body mass index, dialysis before kidney transplant, not presenting with a potential living donor, religious objection to living-donor transplant, and less transplant knowledge were each associated with a lower probability of living-donor transplant.
Race and social determinants of health are associated with the likelihood of undergoing kidney transplant.
与白人患者相比,黑人患者的肾衰竭发病率更高,但接受死亡供体和活体供体肾移植的比例却较低,即使考虑到合并症的差异也是如此。我们评估了健康的社会决定因素(例如人口统计学,文化,心理社会,知识因素)是否可以解释接受死亡供体和活体供体肾移植的种族差异。
设计、地点、参与者和测量方法:我们通过病历回顾,前瞻性地随访了 1056 名接受肾移植(2010-2012 年)的患者,这些患者在肾移植评估后不久完成了一次访谈,直到他们接受肾移植。我们使用多变量竞争风险模型来估计接受任何肾移植、死亡供体移植或活体供体移植的累积发生率,并确定与每种结果相关的因素。
即使考虑到健康的社会决定因素,黑人患者接受肾移植的可能性也较低(亚分布风险比,0.74;95%置信区间,0.55 至 0.99)和活体供体移植(亚分布风险比,0.49;95%置信区间,0.26 至 0.95),但不是死亡供体移植(亚分布风险比,0.92;95%置信区间,0.67 至 1.26)。黑人种族、年龄较大、收入较低、公共保险、合并症更多、在肾脏分配系统更改之前进行移植、宗教信仰更强、社会支持较少、移植知识较少以及学习活动较少,均与接受任何肾移植的可能性降低相关。年龄较大、合并症更多、在肾脏分配系统更改之前进行移植、宗教信仰更强、社会支持较少以及学习活动较少,均与接受死亡供体移植的可能性降低相关。黑人种族、年龄较大、收入较低、公共保险、更高的体重指数、在接受肾移植之前进行透析、没有潜在的活体供体、对活体供体移植的宗教反对以及较少的移植知识,均与接受活体供体移植的可能性降低相关。
种族和健康的社会决定因素与接受肾移植的可能性相关。