Chan Andrew, Rose John, Alvarez Enrique, Bar-Or Amit, Butzkueven Helmut, Fox Robert J, Gold Ralf, Gudesblatt Mark, Haartsen Jodi, Spelman Tim, Wright Katy, Ferraro Diana, Sola Patrizia, Hodgkinson Suzanne, Kalincik Tomas, Lechner-Scott Jeannette, McGuigan Christopher, Spach Karen, Chen Chongshu, Fam Sami, Wu Fan, Miller Catherine
Department of Neurology (AC), Inselspital, Bern University Hospital, University of Bern, Switzerland; Division of Neuroimmunology and Neurovirology (JR), University of Utah, Salt Lake City, UT; Brain Institute (JR), University of Utah, Salt Lake City, UT; Department of Neurology (JR), University of Utah, Salt Lake City, UT; Rocky Mountain Multiple Sclerosis Center at the University of Colorado (EA), Aurora, CO; Department of Neurology and Center for Neuroinflammation and Experimental Therapeutics (AB-O), Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA; Children's Hospital of Philadelphia (AB-O), Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA; Central Clinical School (HB), Monash University, VIC, Australia; Mellen Center for Multiple Sclerosis Treatment and Research (RJF), Cleveland Clinic, OH; Department of Neurology (RG), St. Josef-Hospital, Ruhr University Bochum, Germany; South Shore Neurologic Association PC (MG), Patchogue, NY; Eastern Health MS Service (JH), Box Hill, VIC, Australia; Department of Medicine and Melbourne Brain Centre at the Royal Melbourne Hospital (TS), University of Melbourne, Parkville, VIC, Australia; Department of Neurology and Neurotherapeutics (KW), University of Texas Southwestern Medical Center, Multiple Sclerosis and Neuroimmunology Imaging Program, Clinical Center for Multiple Sclerosis, Dallas, TX; Department of Neuroscience (DF, PS), Neurology Unit, Azienda Ospedaliera Universitaria, Modena, Italy; Liverpool Hospital (SH), NSW, Australia; Department of Medicine (TK), CORe Unit, University of Melbourne, VIC, Australia; Department of Neurology (TK), Royal Melbourne Hospital, VIC, Australia; School of Medicine and Public Health (JL-S), University Newcastle, NSW, Australia; Department of Neurology (JL-S), John Hunter Hospital, Hunter New England Health, Newcastle, NSW, Australia; Department of Neurology (C. McGuigan), St. Vincent's University Hospital and University College, Dublin, Ireland; Envision Pharma Group (KS), Fairfield, CT; and Biogen (CC, SF, FW, C. Miller), Cambridge, MA.
Neurol Clin Pract. 2020 Dec;10(6):510-519. doi: 10.1212/CPJ.0000000000000800.
Delayed-release dimethyl fumarate (DMF) has demonstrated robust efficacy in treating patients with relapsing-remitting multiple sclerosis. Decreases in absolute lymphocyte count (ALC) are a well-known pharmacodynamic effect of DMF treatment, but lymphocyte recovery dynamics are not well characterized after discontinuation of DMF.
Data sources included the Biogen DMF integrated clinical trial data set, a retrospective US chart abstraction study, and data from MSBase. We assessed rate and time course of lymphocyte reconstitution after DMF discontinuation.
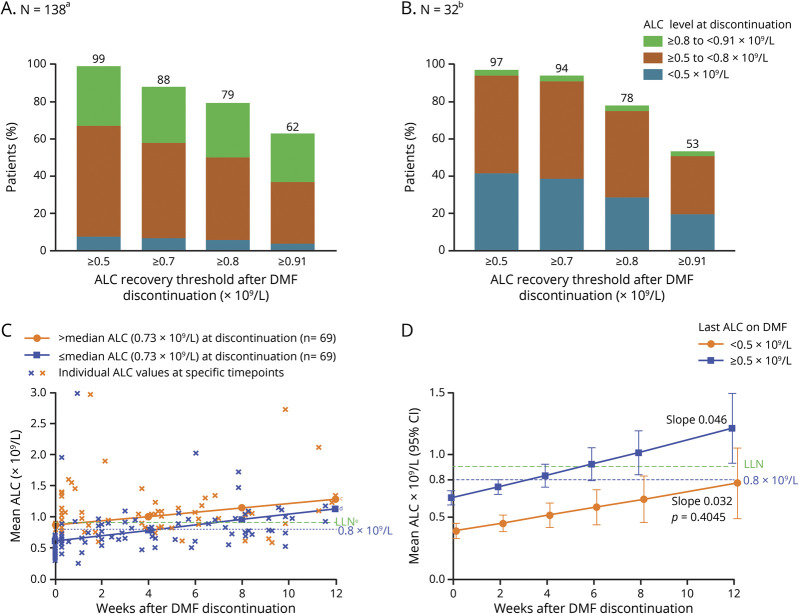
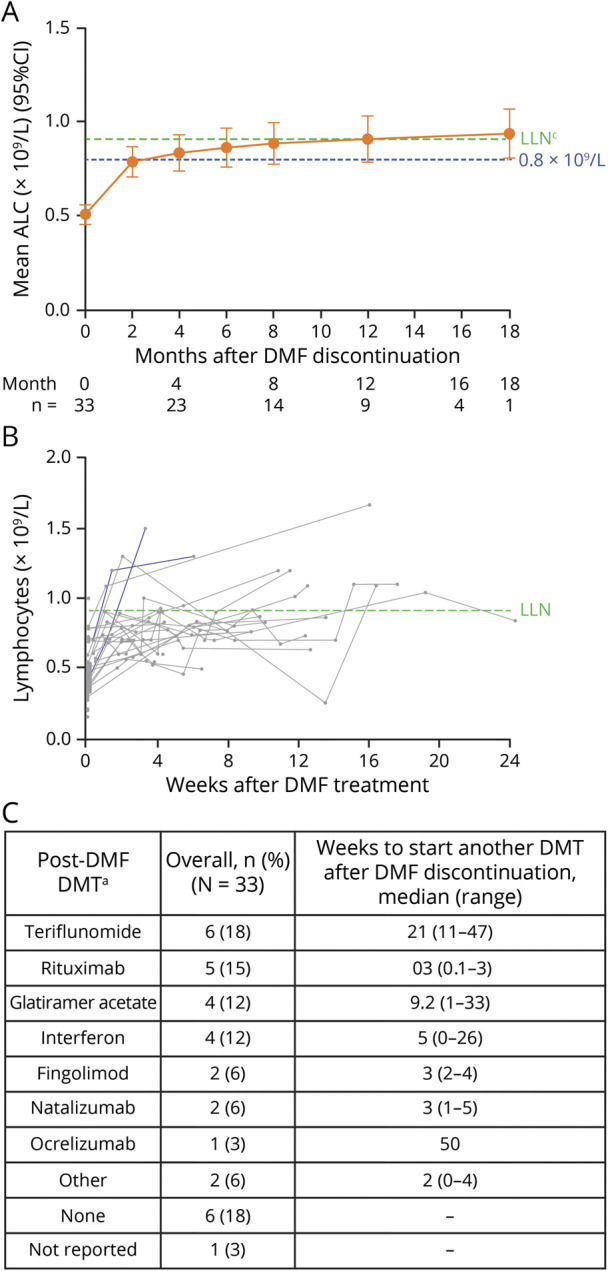
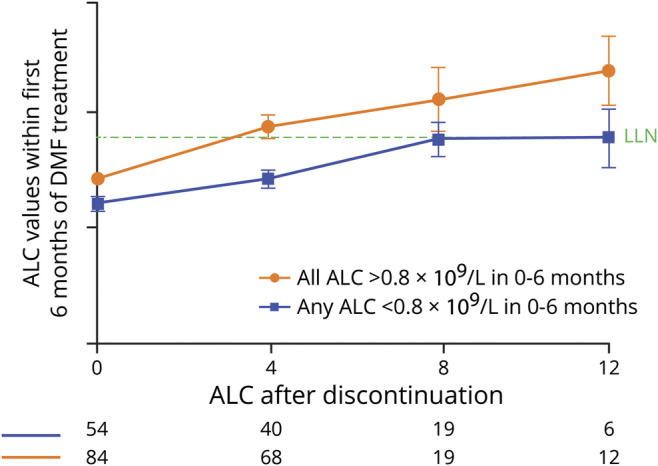
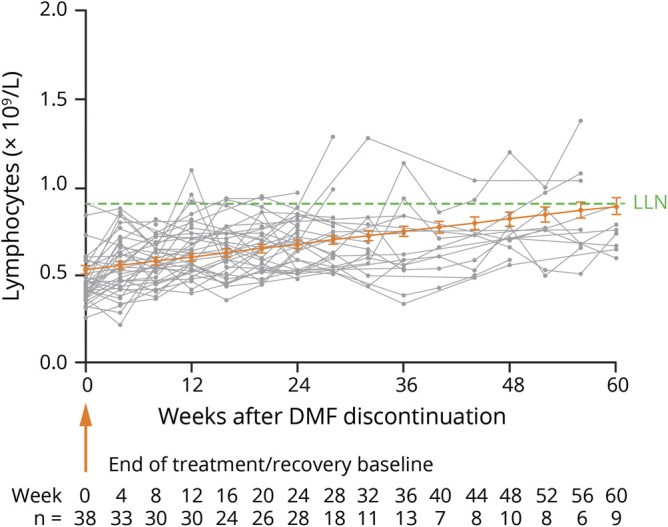
The majority of patients who developed lymphopenia while treated with DMF and subsequently discontinued treatment experienced ALC reconstitution. The median time to reach ALC ≥0.8 × 10/L was 2-4 months after discontinuation for patients treated in real-world data sets; the median time to reach ALC ≥0.91 × 10/L was 2 months after discontinuation in DMF clinical trials. Severity of lymphopenia on treatment and decline in ALC within the first 6 months did not affect the ALC reconstitution rate after DMF discontinuation; rather, on-treatment lymphopenia duration influenced the reconstitution rate. In patients with severe, prolonged lymphopenia for ≥3 years, lymphocyte reconstitution to ≥0.91 × 10/L was 12-18 months vs 2-3 months in patients with lymphopenia persisting <6 months.
The majority of patients who discontinued DMF due to lymphopenia experienced ALC reconstitution within 2-4 months following DMF discontinuation. This may help guide clinicians in managing patients who develop lymphopenia during DMF treatment. Prolonged lymphopenia on DMF treatment is associated with slow lymphocyte recovery after DMF discontinuation.
缓释富马酸二甲酯(DMF)已在复发缓解型多发性硬化症患者的治疗中显示出强大疗效。绝对淋巴细胞计数(ALC)降低是DMF治疗众所周知的药效学效应,但DMF停药后淋巴细胞恢复动态尚未得到充分表征。
数据来源包括百健公司的DMF综合临床试验数据集、一项美国回顾性图表摘要研究以及MSBase的数据。我们评估了DMF停药后淋巴细胞重建的速率和时间进程。
大多数在接受DMF治疗时出现淋巴细胞减少并随后停药的患者经历了ALC重建。在真实世界数据集中接受治疗的患者,停药后达到ALC≥0.8×10⁹/L的中位时间为2 - 4个月;在DMF临床试验中,停药后达到ALC≥0.91×10⁹/L的中位时间为2个月。治疗期间淋巴细胞减少的严重程度以及前6个月内ALC的下降并未影响DMF停药后的ALC重建率;相反,治疗期间淋巴细胞减少的持续时间影响重建率。在严重、长期淋巴细胞减少≥3年的患者中,淋巴细胞重建至≥0.91×10⁹/L需要12 - 18个月,而淋巴细胞减少持续时间<6个月的患者则为2 - 3个月。
大多数因淋巴细胞减少而停用DMF的患者在DMF停药后2 - 4个月内经历了ALC重建。这可能有助于指导临床医生管理在DMF治疗期间出现淋巴细胞减少的患者。DMF治疗期间长期淋巴细胞减少与DMF停药后淋巴细胞恢复缓慢有关。