Smidt Heart Institute, Cedars-Sinai Medical Center, Los Angeles, CA, USA.
National Heart and Lung Institute, Imperial College London, London, United Kingdom.
Cardiovasc Revasc Med. 2022 Jan;34:46-53. doi: 10.1016/j.carrev.2021.01.016. Epub 2021 Jan 22.
Guidelines recommend dual antiplatelet therapy (DAPT) after transcatheter aortic valve replacement (TAVR) but guidelines predate the publication of the largest randomized trial. There have been few trials in the field to date, and with a small number of total patients; pooling their results may therefore be helpful.
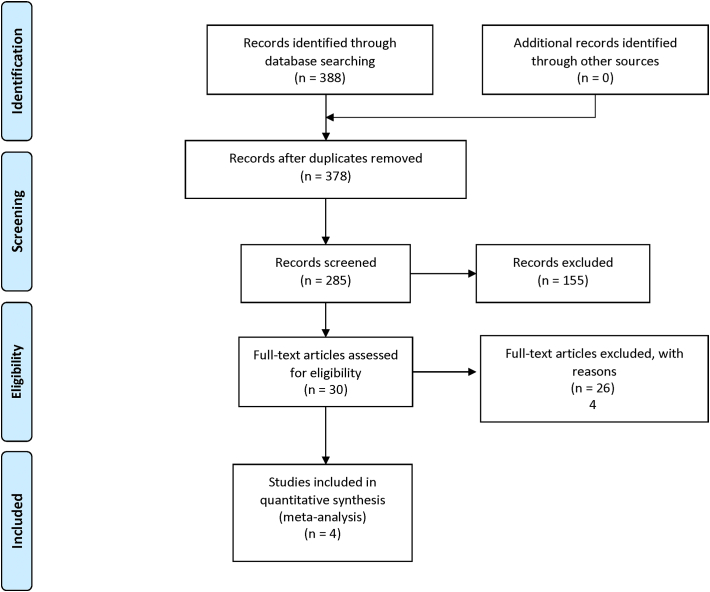
We systematically identified all randomized trials comparing SAPT to DAPT after TAVR. The primary endpoint was the risk of major bleeding. Secondary endpoints included all bleeding, life-threatening bleeding, stroke, myocardial infarction, death and cardiac death.
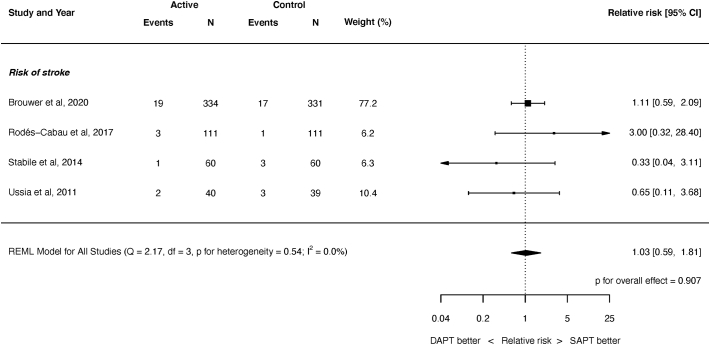
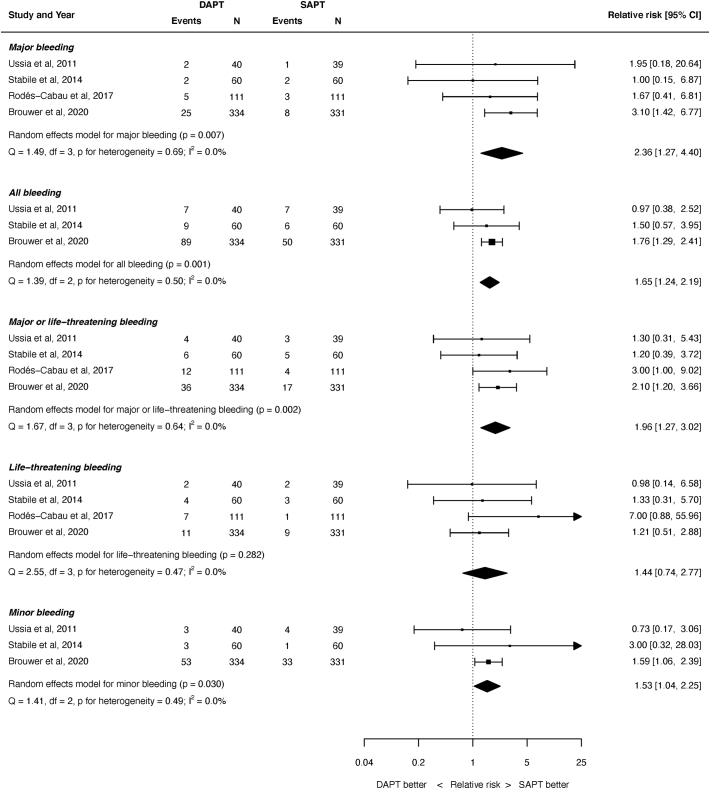
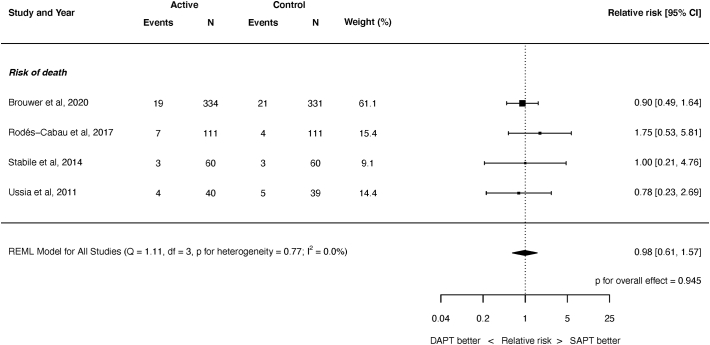
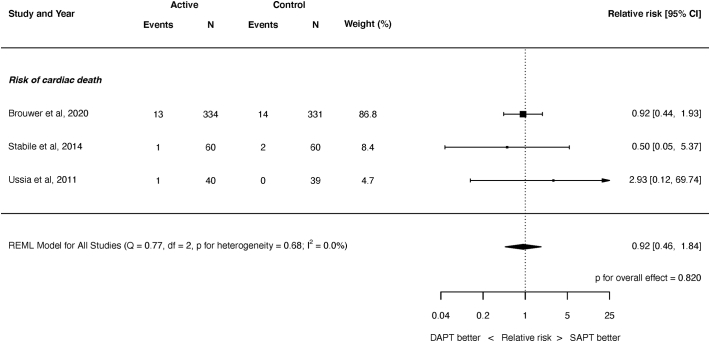
Four trials, randomizing 1086 participants, were eligible (541 randomized to SAPT and 545 randomized to DAPT). The weighted mean follow-up was 9.1 months. The risk of major bleeding was significantly increased after DAPT (relative risk (RR) 2.36, 95% confidence interval (CI) 1.27 to 4.40, P = 0.007). There was a similar increased risk for all bleeding (RR 1.65, 95% CI 1.24 to 2.19, P < 0.001), although not for life-threatening bleeding (RR 1.44, 95% CI 0.74 to 2.77, P = 0.282). There were no significant differences in the risk of stroke, myocardial infarction (MI), death or cardiac death. There was no heterogeneity observed for any endpoint (I = 0.0%).
DAPT after TAVR is associated with an increased risk of major bleeding and all bleeding. There is no evidence of a significant difference between DAPT or SAPT for the risks of stroke, MI, death or cardiac death. However, the total number of patients randomized is small and the duration of follow-up is short. Larger scale randomized trials with longer follow-up are required to assess for any potential differences in ischemic endpoints or mortality.
指南建议经导管主动脉瓣置换术(TAVR)后进行双联抗血小板治疗(DAPT),但指南是在最大规模随机试验发表之前制定的。迄今为止,该领域的试验很少,且总患者人数较少;因此,汇总他们的结果可能会有所帮助。
我们系统地确定了所有比较 TAVR 后短期抗血小板治疗与 DAPT 的随机试验。主要终点是大出血风险。次要终点包括所有出血、危及生命的出血、卒中和心肌梗死、死亡和心脏死亡。
四项试验,共纳入 1086 名参与者,符合入选条件(541 名随机分配至短期抗血小板治疗组,545 名随机分配至 DAPT 组)。加权平均随访时间为 9.1 个月。DAPT 后大出血风险显著增加(相对风险(RR)2.36,95%置信区间(CI)1.27 至 4.40,P=0.007)。所有出血的风险也有类似的增加(RR 1.65,95%CI 1.24 至 2.19,P<0.001),尽管危及生命的出血风险没有增加(RR 1.44,95%CI 0.74 至 2.77,P=0.282)。卒中和心肌梗死(MI)、死亡或心脏死亡风险无显著差异。任何终点均无异质性(I=0.0%)。
TAVR 后 DAPT 与大出血和所有出血风险增加相关。DAPT 与 SAPT 相比,在卒中和 MI、死亡或心脏死亡风险方面没有证据表明存在显著差异。然而,随机患者总数较少,随访时间较短。需要进行更大规模、随访时间更长的随机试验,以评估缺血性终点或死亡率是否存在任何潜在差异。