Division of Nuclear Medicine, Department of Radiology, University of Iowa Hospital and Clinics, Iowa City, Iowa;
Iowa City Virginia Healthcare System, Iowa City, Iowa.
J Nucl Med. 2021 Sep 1;62(9):1274-1277. doi: 10.2967/jnumed.120.254987. Epub 2021 Jan 30.
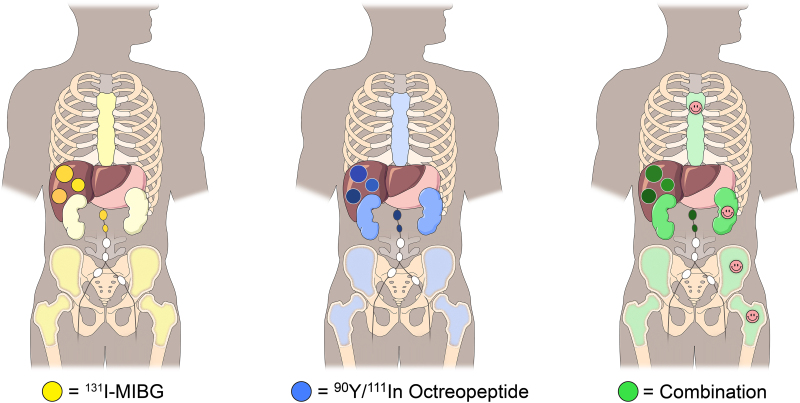
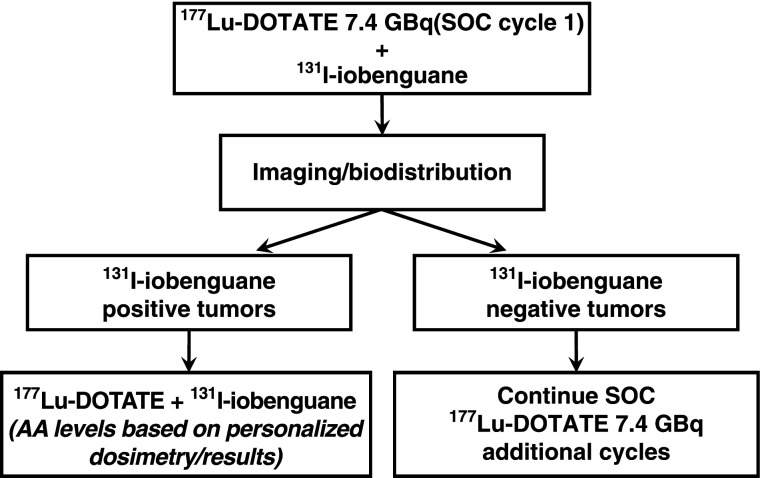
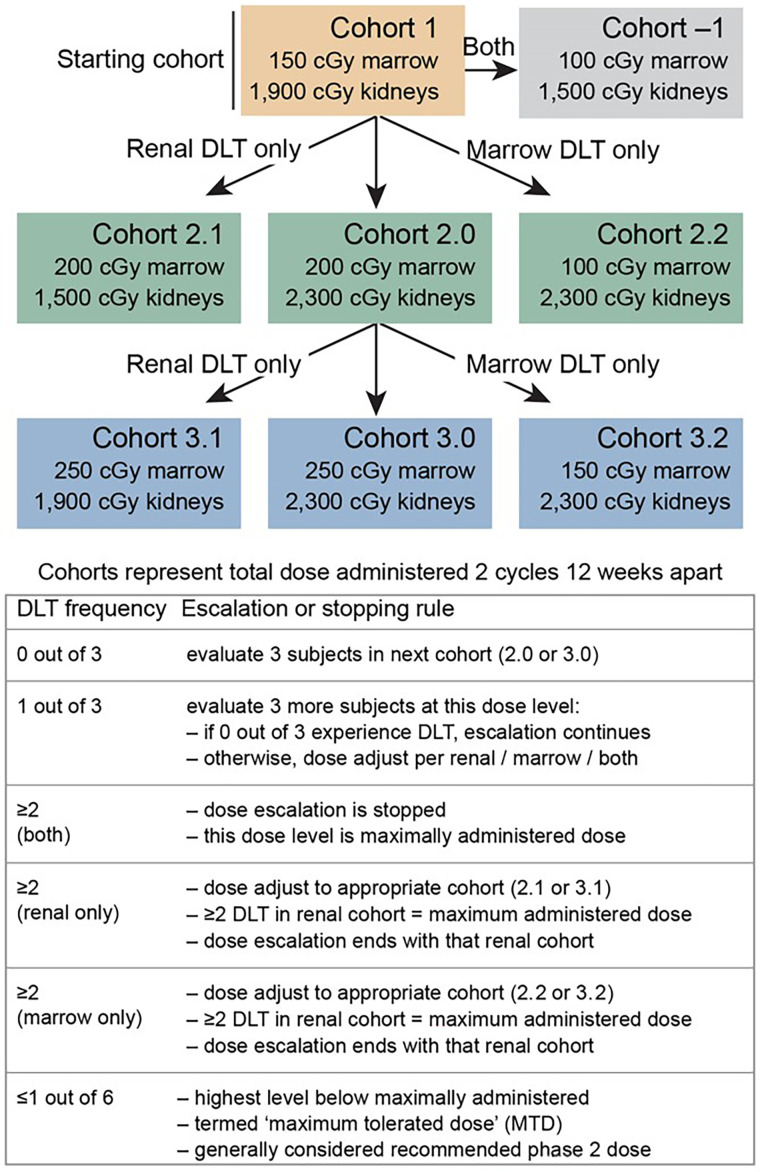
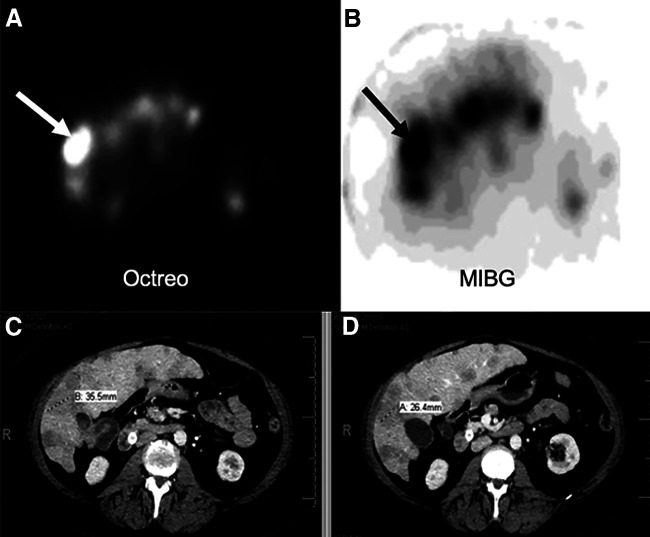
Peptide receptor radionuclide therapy (PRRT) is an effective treatment for metastatic neuroendocrine tumors. Delivering a sufficient tumor radiation dose remains challenging because of critical-organ dose limitations. Adding I-metaiodobenzylguanidine (I-MIBG) to PRRT may be advantageous in this regard. A phase 1 clinical trial was initiated for patients with nonoperable progressive neuroendocrine tumors using a combination of Y-DOTATOC plus I-MIBG. Treatment cohorts were defined by radiation dose limits to the kidneys and the bone marrow. Subject-specific dosimetry was used to determine the administered activity levels. The first cohort treated subjects to a dose limit of 1,900 cGy to the kidneys and 150 cGy to the marrow. No dose-limiting toxicities were observed. Tumor dosimetry estimates demonstrated an expected dose increase of 34%-83% using combination therapy as opposed to Y-DOTATOC PRRT alone. These findings demonstrate the feasibility of using organ dose for a phase 1 escalation design and suggest the safety of using Y-DOTATOC and I-MIBG.
肽受体放射性核素疗法 (PRRT) 是治疗转移性神经内分泌肿瘤的有效方法。由于关键器官剂量限制,提供足够的肿瘤辐射剂量仍然具有挑战性。在这方面,添加 I-间碘苄胍 (I-MIBG) 可能对 PRRT 有利。一项针对无法手术的进行性神经内分泌肿瘤患者的 Y-DOTATOC 联合 I-MIBG 治疗的 1 期临床试验已经启动。根据肾脏和骨髓的辐射剂量限制来定义治疗队列。采用特定于患者的剂量学来确定给予的活性水平。第一队列将肾脏剂量限制在 1900cGy,骨髓剂量限制在 150cGy 以内。未观察到剂量限制毒性。肿瘤剂量学评估表明,与单独使用 Y-DOTATOC PRRT 相比,联合治疗可使剂量增加 34%-83%。这些发现证明了使用器官剂量进行 1 期递增设计的可行性,并表明使用 Y-DOTATOC 和 I-MIBG 的安全性。