CHU de Liège and Centre de Recherche Intégré sur les Médicaments (CIRM), Department of Clinical Chemistry, University of Liège, Domaine du Sart-Tilman, B-4000 Liège, Belgium.
Centre for Research into Cancer Prevention and Screening, Ninewells Hospital and Medical School, University of Dundee, Dundee DD1 9SY, UK.
Nutrients. 2021 Jan 28;13(2):431. doi: 10.3390/nu13020431.
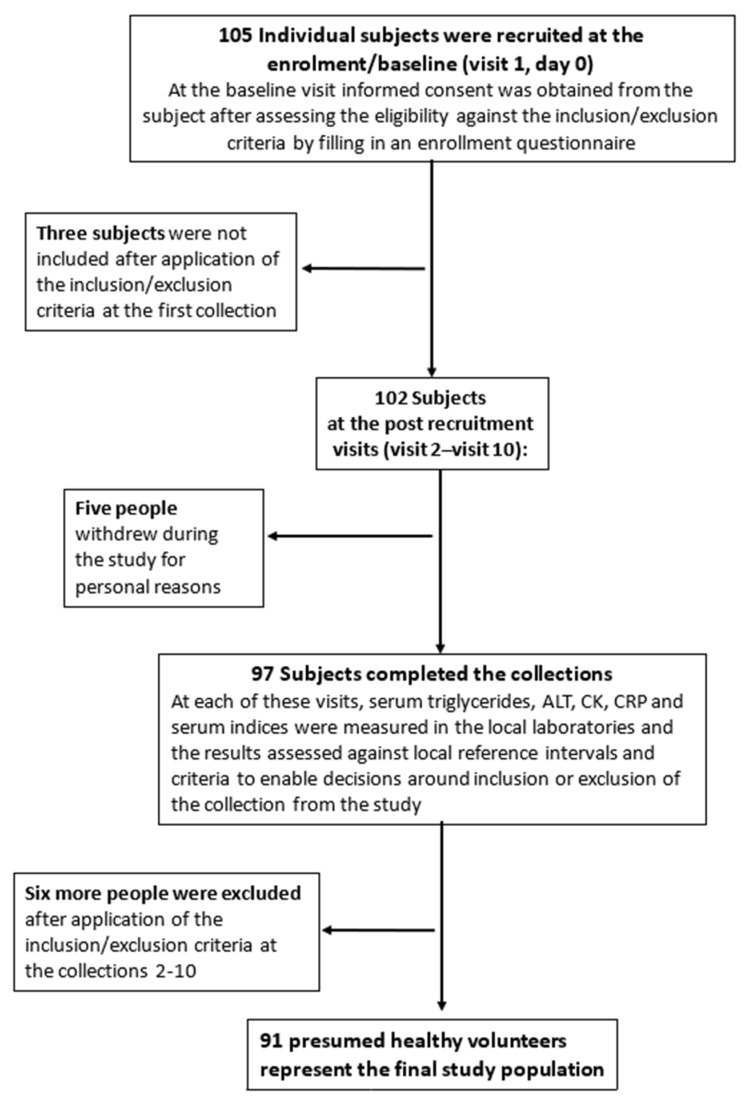
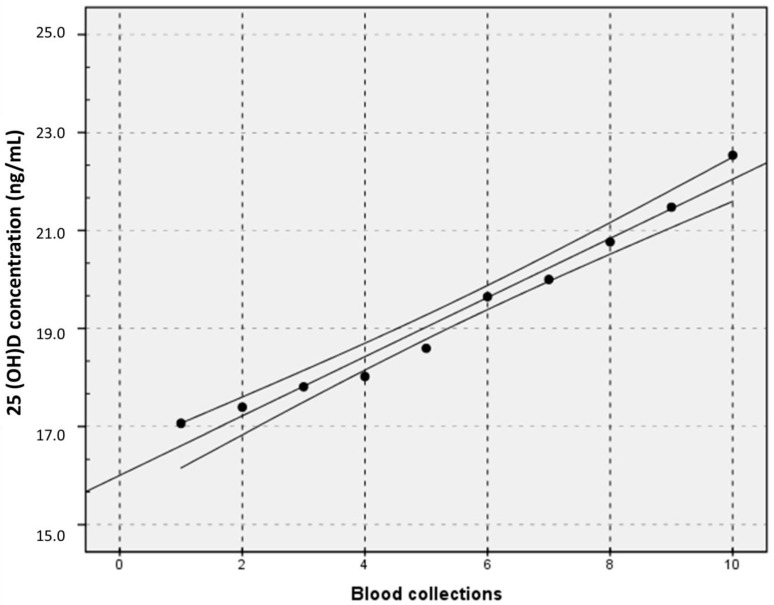
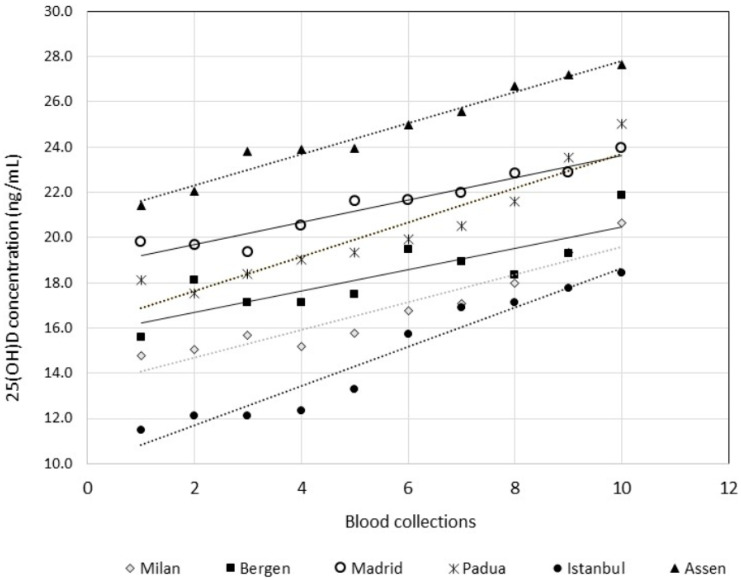
Currently the 25-hydroxy vitamin D (25(OH)D) concentration is thought to be the best estimate of the vitamin D status of an individual. Unfortunately, its measurement remains complex, despite recent technological advances. We evaluated the biological variation (BV) of 25(OH)D in order to set analytical performance specifications (APS) for measurement uncertainty (MU). Six European laboratories recruited 91 healthy participants. The 25(OH)D concentrations in K-EDTA plasma were examined weekly for up to 10 weeks in duplicate on a Lumipulse G1200 (Fujirebio, Tokyo, Japan). The linear regression of the mean 25(OH)D concentrations at each blood collection showed that participants were not in a steady state. The dissection of the 10-sample collection into two subsets, namely collections 1-5 and 6-10, did not allow for correction of the lack of homogeneity: estimates of the within-subject BV ranged from 5.8% to 7.1% and the between-subject BV ranged from 25.0% to 39.2%. Methods that would differentiate a difference induced by 25(OH)D supplementation at < 0.05 should have MU < 13.6%, while at < 0.01, the MU should be <9.6%. The development of APS using BV assumes a steady state of patients. The findings in this study suggest that patients are not in steady state. Therefore, APS that are based on MU appear to be more appropriate.
目前,25-羟维生素 D(25(OH)D)浓度被认为是个体维生素 D 状态的最佳估计。尽管最近技术有所进步,但它的测量仍然很复杂。我们评估了 25(OH)D 的生物学变异(BV),以便为测量不确定度(MU)制定分析性能规格(APS)。六个欧洲实验室招募了 91 名健康参与者。在 Lumipulse G1200 上(Fujirebio,东京,日本),每周对 K-EDTA 血浆中的 25(OH)D 浓度进行两次重复检测,持续长达 10 周。每次采血时平均 25(OH)D 浓度的线性回归表明,参与者未处于稳定状态。将 10 个样本采集分为两个子集,即采集 1-5 和 6-10,并没有纠正缺乏同质性:个体内 BV 的估计值范围为 5.8%至 7.1%,个体间 BV 的估计值范围为 25.0%至 39.2%。区分 25(OH)D 补充引起的差异的方法,在 < 0.05 时 MU 应 < 13.6%,而在 < 0.01 时 MU 应 <9.6%。使用 BV 开发 APS 假设患者处于稳定状态。本研究的结果表明,患者并未处于稳定状态。因此,基于 MU 的 APS 似乎更合适。