Department of Neurology, University of Utah, Salt Lake City, Utah, USA.
Department of Radiology, University of Utah, Salt Lake City, Utah, USA.
J Neurointerv Surg. 2021 Dec;13(12):1128-1131. doi: 10.1136/neurintsurg-2020-016961. Epub 2021 Feb 1.
It has been reported that longer time intervals from stroke onset to endovascular therapy are associated with lower rates of successful reperfusion in acute ischemic stroke patients with large vessel occlusion. However, procedural variables and potential mechanisms of this association have not been fully elucidated.
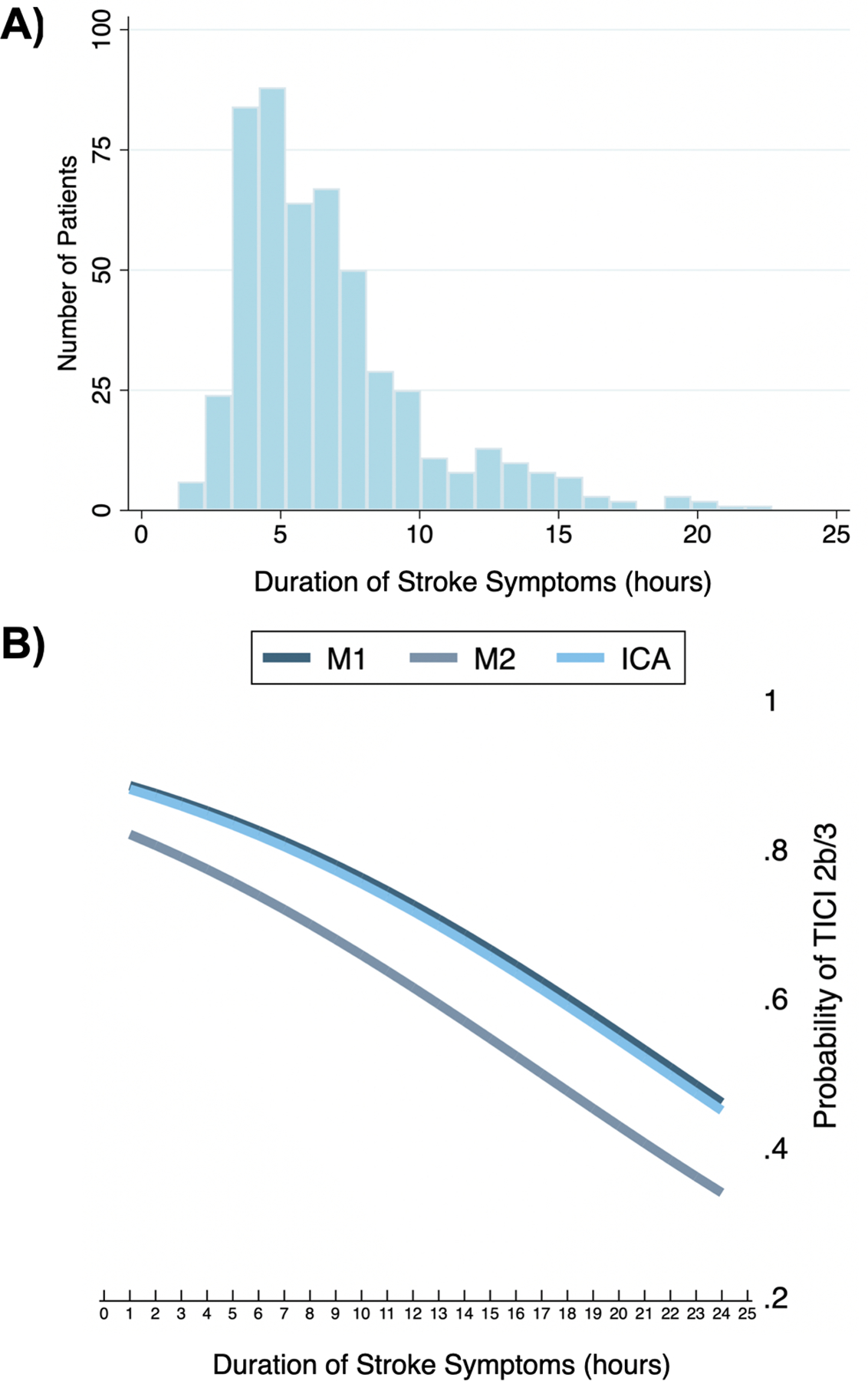
We performed a secondary analysis of individual patient data from the North American Solitaire Stent Retriever Acute Stroke (NASA) and Trevo Stent-Retriever Acute Stroke (TRACK) registries. We included patients with occlusion of the internal carotid artery or middle cerebral artery (M1 and M2 segments) who were treated by mechanical thrombectomy within 24 hours of last known normal. The primary outcome was reperfusion, defined as a Thrombolysis In Cerebral Infarction (TICI) score ≥2b. The secondary outcome was reperfusion on the first pass. The primary predictor was duration of symptomatic stroke, defined as time from last known normal to time of final pass. Adjusted logistic regression models were utilized to determine associations between variables and outcome.
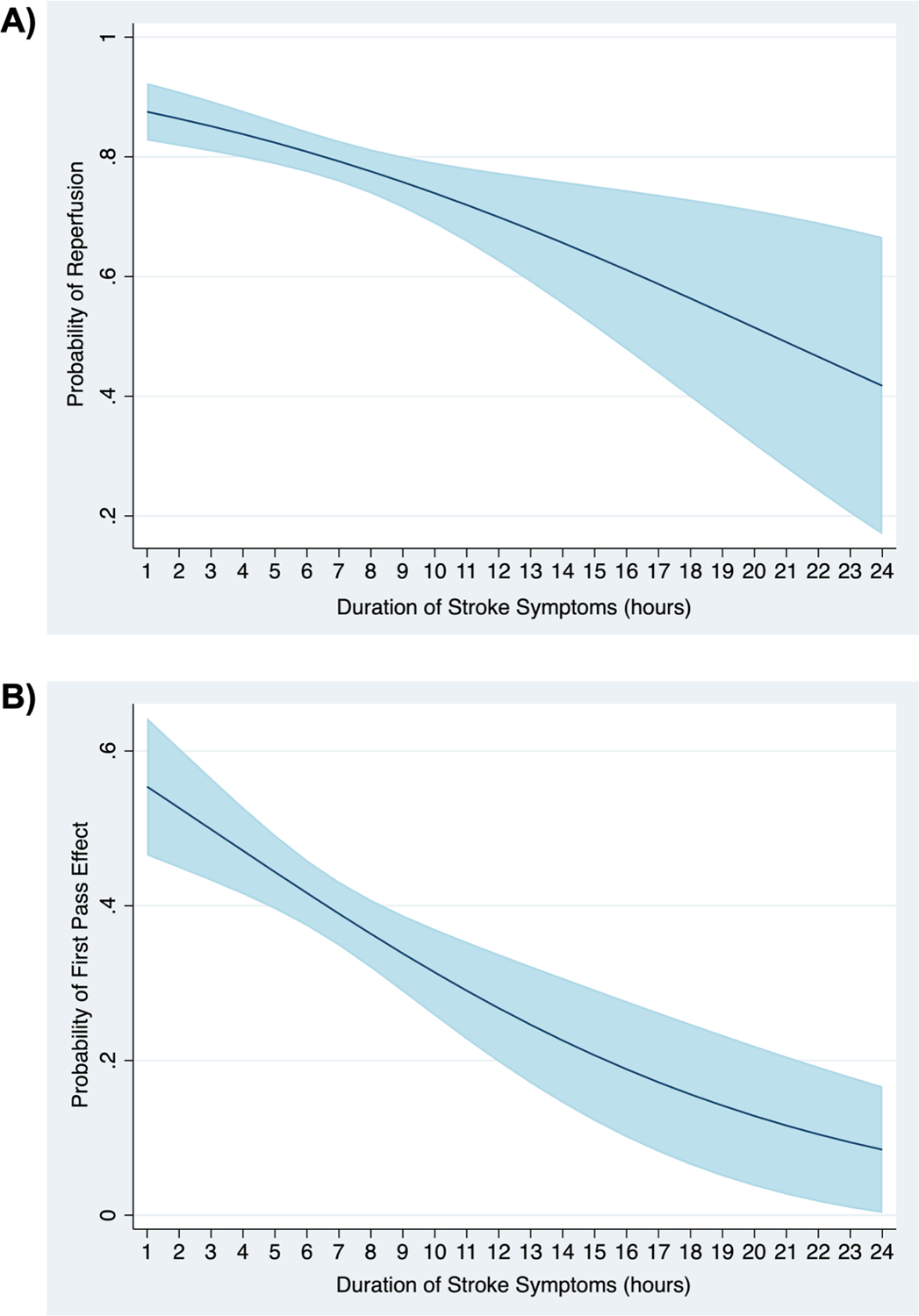
We included 506 patients, of which 401 (79.3%) achieved successful reperfusion (TICI 2b/3). The mean (SD) duration of symptomatic stroke was 6.8 (3.5) hours and in the adjusted logistic regression model the duration of symptomatic stroke was associated with reperfusion (OR 0.90, 95% CI 0.84 to 0.96) and reperfusion on the first pass (OR 0.89, 95% CI 0.83 to 0.95). In that model, the predicted probability of reperfusion was 88% (95% CI 0.83 to 0.92) at 1 hour, 81% (95% CI 0.78 to 0.84) at 6 hours, 70% (95% CI 0.63 to 0.77) at 12 hours, and 42% (95% CI 0.17 to 0.67) at 24 hours (p=0.001). Reperfused patients were significantly younger, more likely to be male, and to have had a balloon guide catheter used during the procedure.
In a real-world cohort of acute ischemic stroke patients with anterior circulation occlusion treated with endovascular therapy, longer duration of symptomatic stroke is associated with lower rates of successful reperfusion and reperfusion on the first pass.
据报道,急性缺血性脑卒中患者大血管闭塞行血管内治疗时,从发病到血管内治疗的时间间隔越长,血管再通率越低。然而,该关联的程序变量和潜在机制尚未完全阐明。
我们对北美 Solitaire 支架取栓急性脑卒中(NASA)和 Trevo 支架取栓急性脑卒中(TRACK)登记处的个体患者数据进行了二次分析。我们纳入了在最后一次已知正常时间后 24 小时内行机械取栓治疗的颈内动脉或大脑中动脉(M1 和 M2 段)闭塞的患者。主要结局为再灌注,定义为血栓溶解治疗脑梗死(TICI)评分≥2b。次要结局为初次通过时的再灌注。主要预测指标为症状性卒中持续时间,定义为从最后一次已知正常时间到最后一次通过时间的时间。采用调整后的逻辑回归模型来确定变量与结局之间的关联。
我们纳入了 506 例患者,其中 401 例(79.3%)达到了成功再灌注(TICI 2b/3)。症状性卒中的平均(标准差)持续时间为 6.8(3.5)小时,在调整后的逻辑回归模型中,症状性卒中持续时间与再灌注(OR 0.90,95%CI 0.84 至 0.96)和初次通过时的再灌注(OR 0.89,95%CI 0.83 至 0.95)相关。在该模型中,1 小时时再灌注的预测概率为 88%(95%CI 0.83 至 0.92),6 小时时为 81%(95%CI 0.78 至 0.84),12 小时时为 70%(95%CI 0.63 至 0.77),24 小时时为 42%(95%CI 0.17 至 0.67)(p=0.001)。再灌注患者明显更年轻,更可能为男性,并且在手术过程中使用了球囊引导导管。
在接受血管内治疗的急性前循环闭塞缺血性脑卒中患者的真实世界队列中,症状性卒中持续时间较长与血管再通率和初次通过时的再灌注率较低相关。